Download
1 / 34
390 likes | 696 Vues
The GI Tract: Secretions, Motility & PONV. Dr James F Peerless October 2013. Objectives. Annex B Physiology & Biochemistry: Gastrointestinal PB_BK_80 Gastric function; secretions, nausea and vomiting PB_BK_81 Gut motility, sphincters and reflex control – neurohumoral integration

E N D
The GI Tract: Secretions, Motility & PONV Dr James F Peerless October 2013
Objectives Annex B • Physiology & Biochemistry: Gastrointestinal • PB_BK_80 Gastric function; secretions, nausea and vomiting • PB_BK_81 Gut motility, sphincters and reflex control – neurohumoralintegration • PB_BK_82 Digestive functions; composition of secretions; digestion of carbohydrates, lipids, proteins, vitamins, minerals Annex C • Applied Physiology & Biochemistry: Gastrointestinal Tract • PB_IK_30 Nausea and vomiting
The GI Tract • Series of organs with specialised functions and characteristic properties • Digestion of ingested food • Absorption of • Water • Nutrients • Electrolytes • Vitamins • Excretion of indigestible and waste products
Gut Motility • Circular and longitudinal muscle • Smooth muscle cells with gap junctions allows for a functional syncytium • Relaxation: rhythmic depolarisation/repolarisation with slow-wave activity • Contraction: spike-burst activity as transmembrane threshold is reached • Frequency and amplitude controlled by nervous and chemical mediators
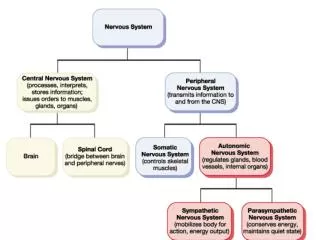
Nervous Control • Intrinsic and extrinsic control • Short and long reflexes • Somatic NS • Pharynx & anus • Autonomic NS • PNS • Vagus – oe prox. colon • S2,3,4 – dist. colon, rectum, anus • SNS • Sympathetic chain
Nervous Control • Local enteric NS • Latticework of plexuses and ganglia within the bowel wall • Auerbach’s (myenteric) plexus • Between long. and circular muscle layers • Neurones classified: • Cholinergic (stim.) • Adrenergic (inh.) • NANC (inh.) • NO, VIP
Control of the Lower Oe Junction • Functional zone of high pressure (15-25 mmHg) 2-4 cm of lower oesophagus • Histologically indistinct • Prevents reflux of gastric contents into Oe • Barrier pressure is the pressure difference between LOS and intragastric pressure • Any decrease in LOS or increase in intragastric pressure increased risk of reflux
Secretions • Main gastrointestinal secretions • mucus and digestive enzymes • Specialisedsecretory cells throughout the gastrointestinal tract, plus liver and pancreas as specialised glands • Secretion stimulated by presence of food in the GI tract, as well as PNS and the intrinsic neuronal control
Saliva • Multifunctional: • Salivary amylase digests starch • Salivary lipase • Buffering and diluting irritants • Aids swallowing, speech and lubricant • Antibacterial: lysozymes, IgA • Serous and mucous mixture: 1000-1500mL day-1 • Parotid - serous • Sublingual and submandibular – both • Buccal – mucus • Regulation • PNS – superior/inf. salivary nuclei • Triggered by taste and touch sensors • Appetite • Reflex salivation by GI irritation
Phases of Gastric Secretion • Cephalic Phase • Thought, sight, smell of food • Vagal stimulation of oxyntic glands and G-cells • Gastric Phase • Vago-vagal reflexes and local enteric reflexes upon food entering the stomach • Release of gastrin • Secretion of acid to pH 2 • Intestinal Phase • Chyme enters small intestine and gastric secretion declines • Lack of stimulation • Inhibitory factors: • Duodenal distension, presence of acid in the duodenum • CCK release
Definitions Nausea is the sensation of the need to vomit Vomiting is the involuntary, forceful expulsion of gastric contents through the mouth Postoperative nausea and vomiting (PONV) is any nausea, retching, or vomiting occurring during the first 24 – 48h after surgery.
PONV • one of the most common causes of patient dissatisfaction after anaesthesia • reported incidences of 30% in all post-surgical patients • up to 80% in high-risk patients • regularly rated in preoperative surveys as the anaesthesia outcome the patient would most like to avoid.
Physiology of Vomiting • Vomiting centre in medulla • CTZ – area postrema (floor of fourth ventricle) • Outside BBB • Multiple receptors (e.g. H1, D2, 5-HT3) • Labyrinth (CN VIII) • Higher cortical centres (fear, sight, smell, memory) • Baroreceptors (CN X) • Pain pathways • GIT chemo- and mechanoreceptors (CN X) • Limbic
Process of Vomiting Pre-ejection Phase Ejection Phase
Process of Vomiting • Pre-ejection Phase • Nausea • SNS stimulation: HR, RR, sweating • PNS stimulation: salivation, relaxation of upper & lower oesophageal sphincters • Retrograde contraction
Process of Vomiting • Ejection Phase • Respiratory pause mid-inspiration • Hyoid and larynx raised to open crico-oesophageal sphincter • Glottis closes • Soft palate elevates to close nasopharynx • abdominal pressure • diaphragm and abdominal muscles contract • Gastro-oesophageal sphincter opens • Ejection of contents
Risk Factors - Patient • Female • Non-smoker • Previous PONV • Hx motion sickness
Risk Factors - Anaesthetic • N2O • Opioids • Etomidate • Neostigmine • Hypotension • both regional and GA
Risk Factors - Surgical • Middle ear surgery • Ophthalmic surgery (esp. strabismus) • Gynaecological procedures
Complications • Unpleasant • Delayed discharge from POCU • Increased length of stay • Suture dehiscence • Aspiration of gastric contents • Oesophageal rupture • Raised intraocular & intracranial pressure • Electrolyte imbalance • Dehydration
Management • Predict the at-risk patient • Multimodal approach • Anaesthetic technique, e.g. TIVA • Local/regional technique • Minimise baseline risk factors, where possible • Minimise peri-operative opioid use • Combine antiemetic use for additive effects