Download
1 / 53
540 likes | 813 Vues
Cleft Lip & Palate imaging. Fetal facial anomalies may be isolated, but most facial abnormalities are associated with more complex fetal malformation syndromes or abnormal karyotypes.

E N D
Fetal facial anomalies may be isolated, but most facial abnormalities are associated with more complex fetal malformation syndromes or abnormal karyotypes. • , when a fetal anomaly is detected,or in high-risk pregnancies a careful ultrasonographicevaluation of the fetal face may also contribute to a specific diagnosis.
EMBRYOLOGY • Facial development begins at about four to five menstrual weeks and is almost complete by the end of the embryonic period, at about 10 menstrual weeks . • the embryo has acquired all its basic morphologic characteristics before the face has attained adequate size to permit ultrasonographic examination. • Most malformations of the face originate from anomalous development of the branchial apparatus, optic vesicles, pharyngeal pouches, and facial prominences, as listed by days after fertilization
ULTRASONOGRAPHIC APPROACH TO THE FETAL FACE AND NORMAL ANATOMY • identified as early as 11 to12 menstrual weeks; but it is usually not until 14 to16 menstrual weeks that the ultrasonographer can observe more detailed facial • the following views should be obtained: • Axial views of the orbits, nose, lips, anterior palate, tongue, and oropharynx • Coronal views of the orbits, nose, lips, maxilla, and anterior portion of the mandible • Profile view of soft tissues and facial bones, including the nasal bones and mandible iv.Views of the ears
a targeted ultrasonographic examination of the face may be particularly useful : • In pregnancies complicated by polyhydramnios, concomitant extrafacial/structural anomalies, a maternal history of teratogen exposure, or a family history of previous craniofacial malformation (e.g., facial cleft) • Visibility may be limited in the presence of oligohydramnios, maternal obesity, or fetal position, especially in the occiput anterior position
three-dimensional ultrasonography (3DUS) has the potential to offer clearer visualization and understanding of fetal facial anatomy. • 3DUS offers the potential advantage of improving visualization of anatomic spatial relations, which is particularly important
Ultrasonographicevaluation also may serve as an indicator of fetal well-being and behavioral changes • For example, fetal vomiting or regurgitation can be identified by watching the fetal mouth, using colorflowimaging to indicate regurgitation in fetuses with upper gastrointestinal obstruction
The sensitivity of ultrasound screening for facial defects in unselected populations has not yet been determined • technologic innovations have improved the accuracy of detecting these abnormalities
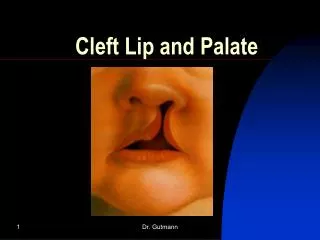
Cleft lip with or without cleft palate is the most common congenital malformation involving the face. • Although often associated, cleft lip and cleft palate are embryologicallyand etiologically distinct malformations, originate at different times during development, and involve different developmental processes . • Cleft lip and cleft palate may be incomplete or complete, unilateral or bilateral,lateralor midline, and symmetric or asymmetric.
The incidence of cleft lip and palate is about 1 per1000 live births in the white population . • a higher prevalence among Asians (1.5–2.0 per 1000) and • Native Americans (3.6 per 1000) and a lower frequency among African-Americans (0.5 per 1000). • About 80% of infants with cleft lip also have cleft palate
There is a high incidence of chromosomal abnormalities among fetuses with facial clefts, in particular trisomy 13 and 18 . • Siblings of patients with cleft lip with or without cleft palate have an increased frequency of cleft lip with or without cleft palate, but not of cleft palate alone; • whereas siblings of patients with cleft palate alone have an increased frequency of cleft palate but not of cleft lip with or without cleft palate . • Cleft lip with or without cleft palate affects male fetuses twice as frequently as females; • , cleft palate alone affects males 25%less than female fetuses.
Etiology Genes • Control cell patterning, cell proliferation, extracellular communication, and differentiation • Clefting usually represents a genetically complex event • Single Mendelian disorders associated with clefting are rare • 2 to 20 genes are thought to interact to result in facial clefting
Some Common Associations, Malformations, and Syndromes Associated with Cleft Lip and Palate • Familial • Chromosomal abnormalities • Trisomy 13/Trisomy 18/Trisomy 21/Trisomy 22/XXXXY syndrome/Various translocations/Triploidy • Autosomal-dominant, autosomal-recessive, and x-linked/cleft syndromes • Multiple syndromes • Nongeneticcleft syndromes • Amniotic band syndrome • Anencephaly • Congenital heart disease • Holoprosencephaly • Encephaloceles • Medial cleft face syndrome • Congenital oral teratoma
Environmental agents • Several agents that are associated with an increased frequency of midfacial malformation. • Medications —phenytoin, sodium valproate, methotrexate. • With corticosteroids there is no evidence of an increase in malformations.
Etiology • Cigarette smoking • Noted with mothers of children with facial clefting, both CL/P and CP. • Alcohol • Associated with an increased risk of fetal facial clefting. • Alterations in cell membrane fluidity or reduced activity of specific enzymes such as superoxide dismutase. • Folate deficiency • Contributes to a range of birth defects. • Evidence is emerging for a similar association with the development of CL/P.
classified clefts into one of five categories. • Type I: cleft lip alone • Type II: unilateral cleft lip and palate • Type III: bilateral cleft lip and palate • Type IV: midline cleft lip and palate • Type V: facial defects associated with amniotic bands or limb–body wall complex
Cleft lip with or without cleft palate results from failure of fusion of the maxillary prominence with the medial nasal prominenceon one or both sides at about the seventh week of development. • The palate forms from the fusion of the primary and secondary palates between the fifth and the 12th weeks. • The secondary palate is the primordium of the remainder of the hard and soft palates and contains the remainingb tooth sockets. It consists of two lateral palatine processes that extend medially and that progressively fuse in the midline from anterior to posterior • . When development is complete, the line of fusion between the primary and thesecondarypalates runs in an arch-like configuration. • Perpendicular to this in the midline, the fusion line of the secondary palate extends from the incisive foramen anteriorly to the uvula posteriorly.
Unilateral Cleft Lip/Unilateral Cleft Lip and Palate • This may reflect the difficulty in diagnosis and the fact that evaluation of the face is not routine in low-risk obstetric ultrasonography • Most clefts detected prenatally with ultrasound are not subtle and tend to be large.
Typicalultrasound features include : • an anechoic region in the upper lip just lateral to the midline, which extends to the nares with a unilateral cleft lip and palate). • a flattened appearance to the affected side, with widening of the nostril and communication between the nostril and the mouth). • nose with a hooked appearance. • A gap in the maxilla and palate. • can be identified as early as 16 weeks’ gestation, • the incomplete cleft lip may be considerably more subtle and not as easily visualized until late in the second or third trimester of pregnancy • The incomplete cleft is visualized best in the coronal view of the lip.
Bilateral Cleft Lip and Palate • identified ultrasonographicallybefore 16 weeks’ gestation • premaxillaryprotrusion,,. The paranasal echogenic mass represents protruding bone and alveolar structures within the premaxillaryprotrusion. The mass typically is inferior to the nose, irregular in shape, and of similar echogenicity to bone and alveolar structures. • categorized bilateral cleft lip and palate into those with premaxillary protrusion and those with a hypoplasticmidface. • Premaxillaryprotrusion is most apparent on midline sagittal views but can also be seen on coronal or transverse views (81).
The differential diagnosis for premaxillaryprotrusionincludes the following: • Anterior cephalocele • Hemangioma • Teratoma • Enlarged protruding tongue • Proboscis (associated with holoprosencephaly)
Cleft Palate • Isolated cleft palate is much more difficult to observe and diagnose ultrasonographically and is frequently missed on prenatal sonograms cleft palate may remain difficult. • These investigators noted that the ability to visualize the anatomy of the hard palate decreased with advancing gestational age; • ultrasonographicassessment should be made before 24 weeks’ gestation. With advancing gestational age, • If a cleft lip is detected, coronal frontal scans obtained more posteriorly and axial views may demonstrate
` • Features suggestive of cleft palate include: • cleft lip, maxillary interruption, and increased tongue excursion . • Color Doppler ultrasound evaluation of the study of nonvascular slow amniotic fluid flow into the nasal andbuccal cavities may be considered a useful diagnostic aid in identification of fetal palate defects • stomach and polyhydramnios may be ultrasonographicclues that the fetus has cleft palate
Median Cleft Lip • The median cleft lip and palate, or premaxillary agenesis, is the rare form and occurs • primarily in association with two syndromes: the median cleft face syndrome (frontonasal dysplasia) and the holoprosencephaly complex
This 3D image demonstrates midline cleft lip and palate (curved • arrow) with hypotelorism and small or near absent nares in this fetus with • alobarholoprosencephaly. O, orbits.
The ultrasonographicfindings: • a gaping midline cleft lip and palate and a hypoplasticmidfacecharacterized by a flattened nose and maxilla • These fetuses have a poor prognosis; • More than half of affected fetuses in this series had either trisomy 13 or trisomy 18.
Amniotic Band Syndrome • also known as the amniotic band disruption complex or limb–body wall complex • , is a common, usually sporadic cause of various fetal malformations involving the craniofacial region, limbs, and trunk. • It is estimated to occur in one in 1200 live births • ranging from mild deformities to severe anomalies that are incompatible with postnatal life
UltrasonographicFindings • Detection of bizarre facial clefts in unusual locations warrants a careful search for other manifestations of the amniotic band syndrome • These include asymmetric encephalocele, gastropleuroschisis, asymmetric amputations, and focal constrictions with distal lymphedema • The facial problems can include cleft lip and occasionally cleft palate, asymmetric microphthalmia, and severe nasal deformity
Sequelaeof the amniotic band syndrome may be observed as early as 12 to 13 weeks’ gestation on endovaginal examination • Identification of a band is not necessary to make the diagnosis, and a diagnosis of amniotic band syndrome • should never be made on observation of these bands in the absence of fetal deformities because several types of membranes may be seen in normal pregnancies