Download
1 / 17
170 likes | 316 Vues
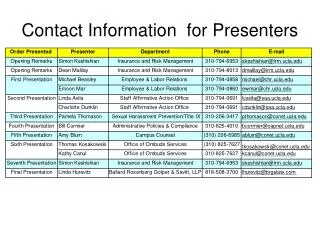
Notes for presenters. This slide set contains a generic training presentation for use by clinicians when training ED staff to support implementation of the London Cardiovascular (LCV) Project NSTEACS pathway.

E N D
Notes for presenters This slide set contains a generic training presentation for use by clinicians when training ED staff to support implementation of the London Cardiovascular (LCV) Project NSTEACS pathway. This template presentation is designed to be tailored for local use. Areas you may wish to edit are highlighted, with suggestions regarding local content. We encourage you to use your Trust’s branded PowerPoint slides.
Notes for presenters The most up-to-date version of this presentation will be hosted on the LCV Project website (www.slcsn.nhs.uk/lcv) plus further information about the project. Questions regarding this presentation or the LCV Project may be directed to info@slcsn.nhs.uk.
High risk NSTEACS patients:Diagnosing and transferring within 24 hours Insert name Trust Date
What we will cover • Need to implement a new pathway for NSTEACS • Pan-London NSTEACS model • Identification of high risk NSTEACS • Management of high risk NSTEACS • What does / will the service look like • Service aims • Inclusion and exclusion criteria • How to access
NSTEACS has a higher mortality at 6 months than STEMI 10 % mortality at six months 8 6 Mortality (%) 4 2 0 0 20 40 60 80 100 120 140 160 180 Need to implement new pathway for NSTEACS ST-segment elevation& depression9.1% (n=1,769) ST-segment depression8.9% (n=4,263) ST-segment elevation6.8% (n=3,369) T-wave inversion3.4% (n=2,723) Days from randomization References: Savonitto et al. JAMA. 1999;281:707.
Pan-London NSTEACS model 999 Patient presents to ED Cardiac cath labNSTEACS centre Angio +/- PCI within 24 hrs (as appropriate) ED diagnosis High risk NSTEACS Rapid assessment
Identification of high risk NSTEACS Patients clinically suspected as having a non-ST elevation acute coronary syndrome (NSTEACS) with ongoing or recurrent chest pain/discomfort believed to be of cardiac origin, together with at least one of the following: • Persistent ECG changes of ST depression >1mm, or transient ST elevation • Pathological T wave inversion in V1-V4 suggesting an ‘LAD syndrome’ • Dynamic T wave inversion >2mm in two or more contiguous leads • Haemodynamic (eg: hypotension, pulmonary oedema or heart failure) or electrical instability (sustained ventricular arrhythmias – VT/VF) which are thought to be due to cardiac ischaemia. • Troponin 0.1mcg/L The above statement should not override clinical judgement. Any NSTEACS patient thought by the admitting hospital staff to be high risk or who potentially may benefit from early angiography/PCI should be discussed with the local cardiologists and, where appropriate, with the regional cardiac centre. A formal risk scoring assessment (eg: GRACE score) should still be undertaken as part of the assessment on all patients admitted with UA/NSTEMI, in line with NICE guidance.
Cardiac enzymes Identification of high risk NSTEACS • Myoglobin (1-3 hours) • Levels peak at 8-12 hours and fall back to normal within 24 hours • CK-MB (3-4 hours) • Peaks at 18-24 hours and returns to normal within 72 hours. • Troponin I and T (3-4 hour) • Remain elevated for 10-14 days
Other reasons for troponin elevation Identification of high risk NSTEACS • Acute PE • Acute pericarditis • Acute or severe HF • Myocarditis • Sepsis and/or shock • Renal failure • Dissecting aortic aneurysm
Identification of high risk NSTEACS A phone call should be made to the receiving hospital, to allow discussion of the appropriateness of early angiography/PCI, taking account of factors increasing the risk of intervention, such as co-morbidities and bleeding risk. If the policy of early intervention/transfer for these patients proves successful then consideration could later be given to agreeing a policy of transfer without prior discussion. Having agreed inter-hospital transfer the referring hospital should initiate an “immediate transfer” with the LAS.
NSTEMI drugs Management of high risk NSTEACS • All ACS patients should get ASA (acetylsalicylic acid) • If the ECG suggest NSTEMI all patients should get clopidogrel • NSTEMI patients should get fondaparinux unless contraindicated
What will / does the service look like?Service aims • Aims to: • Insert the aims of the local NSTEACS centre here
What will / does the service look like? • Insert information about agreed local protocol here
How to access the service • All patients that meet the high risk NSTEACS criteria must be discussed with referral SpR for • Confirmation of appropriateness • Bed status • Ring LAS stating IMMEDIATE transfer
Support is available from the London Cardiac and Stroke Networks Support North Westwww.nwlcn.co.uk020 7009 4075 North Central www.nclcn.org.uk020 3317 3717 North East www.nelcvsn.nhs.uk020 8926 5157 South (includes South West and South East)www.slcsn.nhs.uk020 8812 5950