Download
1 / 82
820 likes | 975 Vues
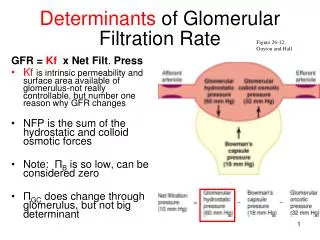
Research Utilization: and its (many) determinants. Carole A. Estabrooks Professor, Faculty of Nursing & Canada Research Chair in Knowledge Translation University of Alberta. University of Melbourne Melbourne, AU October, 2005. Edmonton, Alberta. University of Alberta.

E N D
Research Utilization: and its (many) determinants Carole A. Estabrooks Professor, Faculty of Nursing & Canada Research Chair in Knowledge Translation University of Alberta University of Melbourne Melbourne, AU October, 2005
PARiHS Framework for Research Implementation Evidence-based practice Context Facilitation Evidence PARiHS Model (Kitson, et al., 1998, QSHC
Policy Analysis Framework Policy Framework Lomas, 2000
First…… what do we know about the determinants of research utilization?
Common barriers encountered in knowledge transfer in hospital settings • Commonly identified barriers include: • Time • Resources • Support • Knowledge & skills • Adequate evidence • Culture, context, environment…. • Less commonly identified barriers include: • Disincentives • Irrationality of decision-making environment • Decision-making “errors” • Attitudes & beliefs • Inability to see consequences
Best strategies for transferring research findings? • Imperfect evidence base for decision makers • Many current rigorous evaluations have methodological weaknesses • Poor reporting of study settings, barriers to change, content and rationale of intervention • Generalisability of study findings is frequently uncertain • Reminders most consistently observed to be effective • Educational outreach only led to modest effects • Dissemination of educational materials may lead to modest but potentially important effects (similar effects to more intensive interventions) • Multifaceted interventions not necessarily more effective than single interventions Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay C, Vale L et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess 2004. (Available from: http://www.hta.nhsweb.nhs.uk/)
From some of our work in KUSP In nursing… • Most common interventions tend to be education, protocol & guideline implementation • Little audit & feedback, this is emphasized more among physicians • Individual patient information, personal experience, and social interactions are main information sources • Limited use of journals, textbooks, and other media, including the internet 1
Scott-Findlay’s doctoral work on culture and RU (in progress) • Structure of Authority • Nature of nurses’ work • location of work • expected level of activity • routinized work • expected ways to get work done • Workplace climate • ethical issues • the response to errors • the receptivity to innovation • Types of knowledge valued • clinical knowledge (practical, often tacit) • specialized knowledge (e.g., PICU) • research
Nature of nurses’ work Workplace ethos Manifestations of culture Hierarchical structure of authority Types of knowledge Through ongoing interpretation of events and dialogues members ‘learn’ what is important Intervening factor – inconsistency from superiors that creates unclear expectations Creation of values that result in behavioral expectations Members resort to doing what they are told to do because of inconsistent and shifting expectations Decision not to conform Conformity Scott-Findlay (in progress)
From work in KUSP For interventions we also need to consider (from ethnographic case studies) • Information needs and how these relate to the sources of knowledge used in practice • How the knowledge sources used bear on the packaging and dissemination of “evidence” • How dissemination strategies need to focus on what is needed and useful regardless of what we perceive may be the most relevant approach • A focus on those determinants of research use with the potential to be manipulated in order to develop interventions with potential utility 4
From work in KUSP Organizationally(causal and multi-level modeling) • nursing control over practice • opportunity for nurse-to-nurse collaboration • support for innovation • facilitation of research use • positive culture (characterized by good leadership, evaluation and performance feedback) • increased time to nurse (-ve) • emotional exhaustion (-ve) • Higher nurse education levels • Greater control over practice • Greater freedom to make decisions • Having a good nursing leader on unit • Low levels of emotional exhaustion • A sense of personal accomplishment 5
KUSP Studies • Theorizing the determinants of research utilization (2000 – 2005) • KUPI - The knowledge utilization & policy implementation program (2002 – 2007) • The Bibliometric study (2004 – 2006) • Measuring research utilization (2005 – 2008) • New and future studies
Theorizing the determinants of research utilization (2000 – 2005) Research Utilization Studies The Determinants of Research Utilization: Pain Management in Adults & Children Purpose:To understand how nurses use research in their practice and what influences their ability to use or not use research.
METHODS Ethnographic case studies • Four hospitals (two in Ontario, two in Alberta) • Adult and pediatric surgical units • Qualitative and quantitative data collected • Six months of participant observation each unit • Nurses, patients, physicians, social workers, physiotherapists, and administrators participated
Data Sources • Documents and records • Interviews (individual & group) • Participant observations • Physical artifacts • Measures (e.g., Research utilization, unit culture, critical thinking, pain, workload, environmental complexity)
Quantitative findings (selected - sources only) • In this study the patient care unit was unit of analysis • Our goal: to understand the role of context in shaping RU • We mapped relationship of contextual factors using correspondence analysis
Quantitative findings (cont’d) • Units with highest RU clusteredtogether on factors such as: • Critical thinking • Unit culture • Workload and people support clustered more closely to units with lowest RU scores
Number of Sources Used by Nurses • 20% of nurses use 1 – 5 sources • 50% of nurses uses 6 – 10 sources • 25% of nurses use 11-15 sources
7 Unit Comparison Overall, few differences in the sources used by nurses across units
Sources of Knowledge Patterns Over Time Note. Mean scores were transformed to fit a five-point likert scale (0-4), with 0 as ‘never’ and 4 as ‘always’.
Qualitative findings (selected - sources only) Main Categories of Knowledge Sources • Social interactions • Experience • Documents • Intra-Personal
Why? • Time • Nurses typically work not only on multiple schedules; high and frequent levels of resequencing are required • Context • Nurses tend to be motivated to seek knowledge when they have context specific patient care situations, problems to deal with • Trust • Nurses tend to seek information , knowledge from those they trust (knowledgeable, empathetic) • Hierarchy • An environment where norms of organizational hierarchy are strictly adhered to may negatively affect knowledge transfer between nurses and CNS’s, clinical leaders, and physicians.
Summary & Conclusions • Individual patient information, personal experience, and social interactions are main information sources • Limited use of journals, textbooks, and popular media, including the internet • The structure and organization of nurses’ work has a major influence on their choice of knowledge sources • Researchers need to merge nurses’ information-seeking behavior with dissemination strategies
Summary & Conclusions • The nurses in this study overwhelmingly relied on social interactions and experience as their primary sources of practice knowledge • Time, trust, and unit environment played an important role in determining the nurse’s sources of knowledge
KUPI: The knowledge utilization & policy implementation program (2002 – 2007)
Evidence-based practice • PARISH Promoting Action on Research Implementation in Health Services • SI = f (E,C,F) Successful implementation is a function of evidence, context and facilitation Kitson et al, 1998 Rycroft-Malone et al, 2002 Context Facilitation Evidence
Knowledge utilization and policy implementation(KUPI) A five year research program whose purpose is to develop theory in the knowledge utilization field that increases (research) knowledge use by clinicians and decision-makers across multiple levels - by using existing data
Objectives of the larger KUPI program To study: • how predictors of research use vary across levels of decision-making • how research use is accomplished in organizations, and • how research use shapes policy implementation
Modeling Sub-Projects Designed to study factors influencing knowledge use, specifically research utilization (RU), at different levels of decision-making among nurses in Alberta hospitals.
Modeling sub-project: Five studies • DV derivation & outcome validation • A structural equation (SEM) assessment of the PARiSH (Kitson) model • Multi-level (HLM) modeling • Hierarchical structural equation modeling (H-SEM) • A methodological evaluation of HLM vs. H-SEM and their usefulness for the study of research utilization
Example: Multi-level (HLM) study objectives • To determine which nursing factors at the individual, unit, and hospital levels predict research utilization • To measure the contribution of the significant factors to variation in research utilization across units and hospitals
The Alberta Nurse Survey (1998) A census population of all 12,345 registered nurses from 129 hospitals in Alberta, Canada. Useable returns 6526 (52.8%) A:Employment Characteristics B: Nursing Work Index (NWI) C: Maslach Burnout Inventory(MBI) D: Job characteristics E: Last shift F: Demographics G: Site specific questions
The Research Utilization Survey (1996) A randomly selected sample of staff nurses in Alberta, Canada. Useable returns 600 (42%) • Research utilization • Background and daily demands • Individual and professional factors • The research itself • Your organization
Final Sample HospitalsNurses 109 6,526 90 5,228 Selection criteria: 5 nurses per hospital
The 3 level model Organization factors (hospital level) Specialty factors (unit level) Nurse factors (individual level)
Significant univariate predictors: Individual, specialty (unit), and hospital levels Individual level • Higher nurse education • Control over practice • Freedom to make decisions • Emotional exhaustion • Lack of personal accomplishment Specialty (unit) level • Leadership • Relational capital • Consulting opportunity • Participate in policy Organizational level • Climate • Innovativeness • Organizational slack
Summary Greater research utilization among nurses was predicted in the final model by: • Higher nurse education levels • Greater control over practice • Greater freedom to make decisions • Having a good nursing leader on unit • Low levels of emotional exhaustion • A sense of personal accomplishment
Components (%) of research explained at the individual, specialty (unit), and hospital levels 4.5% 3.7% 91.8%
Summary Variation in research utilization was mainly due to differences in individual characteristics of nurses, with organizational factors contributing less. Of the latter, however, having good leadership on the unit was the most significant determinant of research utilization
Structural equation (SEM) modeling objective • to develop a theoretical model of hospital characteristics that predict research use by nurses
Innovation Facilitation Hospital Size Nursing Education Staff Development Programs Responsive Administration Control over Practice Nurse to Nurse Collaboration RU Relational Capital Time to Nurse Internet Use Staffing and Support Services Emotional Exhaustion The Structural Equation Model (SEM)
Structural Equation Modeling Results • Positive impact on research use: • nursing control over practice • opportunity for nurse-to-nurse collaboration • support for innovation • facilitation of research use • positive culture (characterized by good leadership, evaluation and performance feedback) • Negative impact on research use: • Increased time to nurse • emotional exhaustion