Download
1 / 33
330 likes | 553 Vues
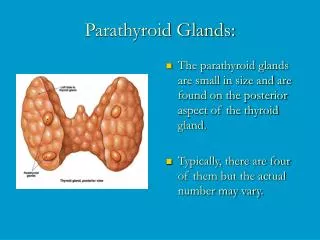
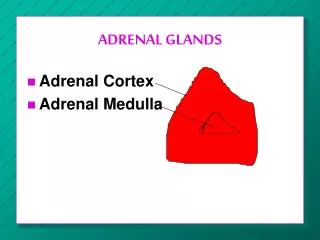
SUPRARENAL GLANDS DISEASES. L ecturer : Sakharova I.Ye. M.D. A Close Look at the Adrenal Glands. Adrenal glands hyperfunction:. Adrenal glands hypofunction:.

E N D
SUPRARENAL GLANDS DISEASES Lecturer: Sakharova I.Ye. M.D.
Cushing's syndrome is a multisystem disorder resulting from chronic exposure to inappropriately elevated concentrations of free circulating glucocorticoids.
Etiology of Cushing's syndrome Endogenous(ACTH dependent 85%) • Cushing's disease (pituitary) • Ectopic ACTH syndrome (small cell lung carcinoma) • Ectopic CRH syndrome (bronchial carcinoid tumours) ACTH independent 15% • Common:Adrenal adenoma, adrenal carcinoma • Less common:Micronodular hyperplasia, macronodular hyperplasia • Rare:McCune-Albright syndrome, gastric inhibitory polypeptide
Exogenous • ACTH treatment • Glucocorticoid treatment Pseudo-Cushing's syndrome • Major depressive disorder • Alcoholism • Obesity
Clinical features of Cushing's syndrome • 90% - Central (truncal) obesity. Fat deposits may appear in the cheeks (moon facies), in the dorsocervical area (buffalo hump), and the supraclavicular area • 85% - Hypertension • 65% - Presence of multiple purple striae with a diameter >1 cm on the abdomen or proximal extremities • 60% - Muscle wasting and weakness affect the proximal muscles of leg and shoulder girdle • 40% - Easy bruising of the skin • 40% - Osteoporosis
Hyperpigmentation (palmar creases and pressure points) in a patient with Cushing's syndrome strongly suggests an ACTH cause (Cushing's disease) • Patients may have mild hirsutism and acne, but severe hirsutism and especially virilisation strongly suggest an adrenal carcinoma. • Depression, lethargy, and insomnia often occur at the same time as other symptoms. In children the dominant clinical features are cessation of linear growth and weight gain; the clinical course is more aggressive than in adults.
Investigation of Cushing's syndrome Screening tests (outpatient) • Urinary free cortisolThe measurement of 24 hour excretion of cortisol in urine integrates the variations in plasma free cortisol concentrations seen during the entire day; three consecutive 24 hour urine specimens. There is a false negative rate of 5.6%, with false positives of 1% in normal people and 5% in obese individuals.
Dexamethasone suppression tests In normal subjects, administration of a supraphysiological dose of glucocorticoid results in suppression of ACTH and hence of cortisol secretion (cortisol <50 nmol/l). This is the basis of dexamethasone suppression tests, of which there are several types.
The 48 hour low dose test, which is the most sensitive and specific screening test, entails the administration of 0.5 mg dexamethasoneat intervals of exactly 6 hours from 9 am on day one for eight doses, and measurement of serum concentrations of cortisol at 9 am on day three, exactly 6 hours after the last dose of dexamethasone. A negative result is indicated when the serum concentration of cortisol at 9 am on day three is suppressed to < 50 nmol/l.Over 98% of patients with Cushing's syndrome fail to "suppress" serum cortisol on the low dose test.
Confirmatory tests • Insulin tolerance testIn normal subjects and those with pseudo-Cushing's, insulin induced hypoglycaemia (blood glucose concentration <2.2 mmol/l) results in a rise of ACTH and cortisol concentrations. This response to hypoglycaemia is lost in most cases of Cushing's syndrome (90%). This test is contraindicated in anyone with a history of epilepsy or cardiac disease and in those with hypothyroidism and hypoadrenalism.
Treatment of Cushing's syndrome • Transsphenoidal surgery • Pituitary radio-therapy • Bilateral or unilateral adrenalectomy • Medical therapy
Medical therapy • Metyrapone and ketoconazole are commonly used. Metyrapone blocks the 11-ß hydroxylase enzyme involved in the final step in cortisol synthesis, whereas ketoconazole acts at several levels and inhibits cortisol synthesis by a direct action on the P450 cytochrome enzyme. The adrenolytic agent, mitotane, has a cytotoxic effect on both normal and malignant adrenocorticol tissue. Its use is mainly in the management of adrenal carcinoma and rarely in Cushing's disease.
Conn's syndrome is a disease of the adrenal glands involving excess production of a hormone, called aldosterone. Another name for the condition is primary hyperaldosteronism.
Epidemiology of Conn's syndrome • Represents under 1% of hypertension causes • Peak age 30-50 years • Most patients are women
Primary Hyperaldosteronism (Conn's syndrome) • Solitary adrenal adenomas (80-90%) • Bilateral adrenal hyperplasia (10-20%) 3. Adrenal Carcinoma (rare) 4. Unilateral Adrenal Hyperplasia (very rare)
Clinical features of Conn's syndrome • Often asymptomatic • Frontal headache • Muscle weakness to flaccid paralysis decreased muscle strength (because of low potassium level) • Polyuria and Polydipsia (carbohydrate intolerance) • Hypertension
Investigation of Conn's syndrome • Serum Electrolytes • Serum Potassium decreased • Serum Sodium increased (Mild) • Metabolic Acidosis B. Increased serum level of aldosterone C. Greatly decreased serum level of renin Blood may also be taken directly from the adrenal veins (via a catheter passed through a vein in the inguinal region) to determine whether both adrenals are over-secreting aldosterone.
Treatment of Conn's syndrome • Adrenal Adenoma • Surgical excision (unilateral adrenalectomy) B. Adrenal Hyperplasia • Spironolactone (Aldactone)
Congenital adrenal hyperplasia (CAH) is a group of inherited autosomal-recessive disorders in which a genetic defect results in the deficiencyof an enzyme essential for synthesis of cortisol and, attimes, aldosterone.
The incidence of CAH is 0.06 to 0.08 in 1,000 live births.There are several forms of CAH, the most common of whichis 21-hydroxylase (21-OH) deficiency, occurring in over 90%of all cases (AAP, 2000).
Pathophysiology • In a child with CAH, cortisol synthesis is blocked by the lackof the enzyme 21-OH. This reduction of cortisol leads ton increased ACTH production by the anterior pituitary.Prolonged oversecretion of ACTH causes enlargement orhyperplasia of the adrenal glands and excess production ofandrogens.
Clinical features of CHA • The enzyme deficiency of 21-OH exposes the fetus to excessiveproduction of androgens. In the male fetus, this causesno physical changes; however, in the female, excessiveandrogens will virilize (to develop sexual characteristics of amale) the external genitalia, resulting in an enlarged clitoris(possibly to the extent of resembling the male phallus),fusion of the labial folds, and a rugated appearance to thelabia. This is known as ambiguous genitalia or pseudohermaphrodism.The ovaries, fallopian tubes, and uterus arenormal.
Approximately 75% of cases of 21-OH deficiency havesalt wasting from a defect in ability to synthesize aldosterone.If not diagnosed at birth, the neonate with 21-OHdeficiency and salt wasting will develop a life-threateninghyponatremia, hyperkalemia, and hypovolemia by day 10-14of life. This is known as adrenal crisis.
Acute adrenal (addisonian) crisis • Clinical features –fever, dehydration, nausea, vomiting, hypotension, that evolves rapidly to circulatory shock.
Treatment of acute adrenal (addisonian) crisis • Hydrocortison (Cortef) IV 100 mg as a bolus • Intravenous saline and glucose • Hydrocortison 10-15 mg/kg as a continuous infusion for 24 hours Decrease one third of the hydrocortison daily dose every day until a maintenance dosage is reached within 5 days
Children with atypical 21-OH deficiency will presentlater (often in the toddler or preschool years) with prematureadrenarche (pubic hair development), acceleratedgrowth velocity,advanced bone age, acne, and hirsutism(excessive body hair in a masculine distribution pattern).
Investigation of CAH • Molecular genetics • Increased level of 17-hydroxyprogesteron in serum • Increased level of 17-ketosteroids in urine • Positive reaction to the glucocorticoid-therapy