Download
1 / 27
270 likes | 470 Vues
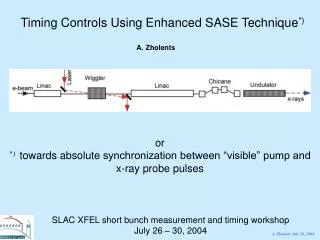
Surgery in acute colitis timing and technique. Bruce D George John Radcliffe Hospital. Acute Severe Colitis. Truelove and Witts criteria Diarrhoea: over 6/day Macroscopic blood in stool and Temperature over 37.5 or Tachycardia over 90/min or Anaemia less than 10.5g/dl or

E N D
Surgery in acute colitistiming and technique Bruce D George John Radcliffe Hospital
Acute Severe Colitis • Truelove and Witts criteria • Diarrhoea: over 6/day • Macroscopic blood in stool • and • Temperature over 37.5 or • Tachycardia over 90/min or • Anaemia less than 10.5g/dl or • ESR over 30mm/hour
Hardy and Bulmer 1933 95 cases, Birmingham 75% mortality in first year after first presentation History of severe UC
210 patients, 109 cortisone, 101 placebo 41% vs 16% remission p<0.01 7% vs 24% mortality during first attack
High dose steroids (and cyclosporin) Joint medical and surgical care regular clinical and radiological assessment Total colectomy + ileostomy five day rule Very low mortality The Current Position
Predictors of outcome • Bowel frequency • Pulse>100/min • Max temp >38 • Albumin < 30g/l on day 4 • Mucosal islands on AXR • Toxic dilatation
If on Day 3 : > 8 stools per day or 3-8 stools per day + CRP >45mg/l 85% chance of colectomy Predicting outcome in severe ulcerative colitisTravis et al 1996
The standard Operation • Total colectomy • End ileostomy • Rectal stump
Joint medical and surgical management Early surgery for non-responders Very low mortality Key principles
John Radcliffe Hospital 1994 to 2000 81 patients (41 female, 40 male) Median age 34 years (range 10-80) Median follow-up 5.4 years (range 1.1 to 10) Colectomy for severe acute colitis(presumed UC)
Major surgical Small bowel obstruction 9 Rectal stump complications 5 Wound 2 Miscellaneous 2 Major medical 5 Total 28% Complications of Acute Colectomy
Further surgery Pouch 57 (70%) Completion proctectomy 13 (16%) No restoration/completion 11 (14%) But that is only the beginning
Unplanned re-admission 40 (49%) Major surgical 41 (51%) Small bowel obstruction 22 (24%) Requiring re-operation 8 (10%) Major medical 10 Mortality 0 Cumulative morbidity in JR series
Alves et al 2003 164 patients Mortality 0.6% (0%) Morbidity 33% (28%) Re-op for SBO 8% (10%) Complications of acute colectomy
MacLean et al 2002 1178 patients undergoing pouch reconstruction Median follow-up 8.7 years 351 episodes of SBO in 272 patients (23%) (24%) Loop ileostomy identified as risk factor Small bowel obstruction
Blame the drugs Operate on fewer patients Make the surgery better How to do better?
Steroids (any dose) 5.54 (1.12-27) <20mg 6.28 (0.97-40) 20-40mg 5.87 (0.9-38) >40mg 18.94 (1.72-207) AZA/6MP (any dose) 1.2 (0.37-3.94) Aberra et al 2003 Odds ratios for major surgical complications of IBD surgery
Does cyclosporin add to surgical morbidity? • Hyde et al DCR 2001 • 44 patients colectomy for severe UC
Cyclosporin McCormack et al DCR 2002 46 patients failed response to 7 days high dose steroids 14 (30%) no effect (colectomy) 32 (70%) initial response Early relapse in 9 (20%) [colectomy] Sustained response in 12 (26%) Operate on fewer patients
Non-responders Partial responders ?improve on pre-attack therapy ?convert to elective surgery Responders Operate on fewer patients
2001 British DGH 32 episodes in 25 patients (1994-2000) Median age 36 years (17-81) 6 died (24% mortality) 3 post-op, all surgery > day 10 But don’t delay inappropriately
Management of the rectal stump Anti-adhesion strategies Laparoscopic Make the surgery better
Tissue separation Sodium hyaluronate based bioresorbable membranes (Seprafilm) Icodextrin 4% (Adept) Anti-adhesion Strategies
Long operating times Less pain Earlier return of bowel function Shorter hospital stay Similar morbidity Marcello et al (DCR 2001) 16% vs 24% Bell (Surg Endosc 2002) 33% Laparoscopic colectomy for acute severe colitis ? Reduced small bowel adhesions
The current gold standard Is it good enough? Send fewer patients along surgical path Make the surgical path less hazardous Summary