Download
1 / 43
480 likes | 748 Vues
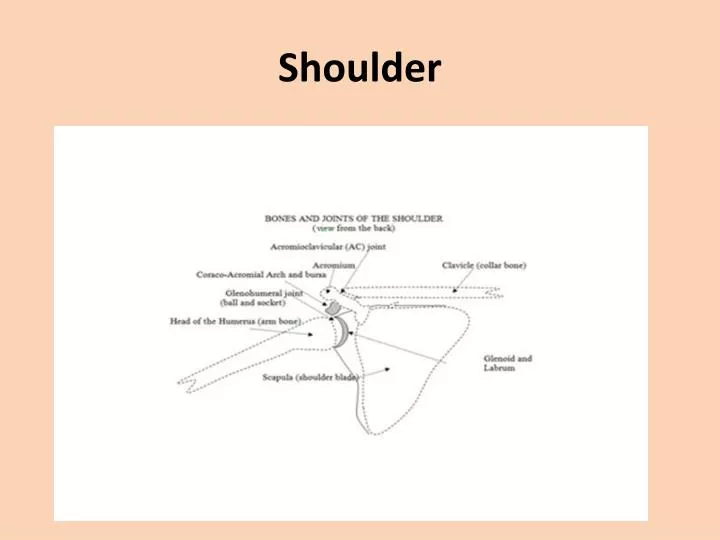
Shoulder. 30 Muscles involved in the Shoulder . Who is this?. What record did he set?. How many yards?. 5,476. 40,762 ? 2, 383 ?. Passing Yards in a Career. 1. Brett Favre 71,838 1991-2010 4TM 2. Dan Marino+ 61,361 1983-1999 mia 3. Peyton Manning (35) 54,828 1998-2011 clt

E N D
5,476 40,762 ? 2, 383 ?
Passing Yards in a Career • 1. Brett Favre 71,838 1991-2010 4TM • 2. Dan Marino+ 61,361 1983-1999 mia • 3. Peyton Manning (35) 54,828 1998-2011 clt • 4. John Elway+ 51,475 1983-1998 den • 5. Warren Moon+ 49,325 1984-2000 4TM • 6. Fran Tarkenton+ 47,003 1961-1978 2TM • 7. VinnyTestaverde 46,233 1987-2007 7TM • 8. Drew Bledsoe 44,611 1993-2006 3TM • 9. Dan Fouts+ 43,040 1973-1987 sdg • 10. Kerry Collins (39) 40,922 1995-2011 6TM • 11. Drew Brees (32) 40,742 2001-2011 2TM • 12. Joe Montana+ 40,551 1979-1994 2TM • 13. Johnny Unitas+ 40,239 1956-1973 2TM • 14. Tom Brady (34) 39,979 2000-2011 nwe
Symptoms • Painful popping, clicking, or “catching” in the shoulder • Pain when attempting to extend the arm overhead or reach behind the back • Pain when throwing a ball • An aching pain felt deep in the shoulder
SLAP Tear • Superior Labrum from Anterior to Posterior. • The SLAP tear occurs at the point where the tendon of the biceps muscle inserts on the labrum.
SLAP Tear • A SLAP tear is an injury to a part of the shoulder joint called the labrum. • similar to the hip; however, the socket of the shoulder joint is extremely shallow, and thus inherently unstable. • To compensate for the shallow socket, the shoulder joint has a cuff of cartilage called a labrum that forms a cup for the end of the arm bone (humerus) to move within.
Etiology • Fall onto an outstretched hand • Repetitive overhead actions (throwing) • Lifting a heavy object • The area of the labrum where the SLAP tear occurs is susceptible to injury because it is an area of relatively poor vascularity. Other parts of the labrum often heal more easily because the blood supply delivers a healing capacity to the area of the tear. • In the area of SLAP tears this is not the case, and chronic shoulder pain can result.
Clumsy • a slip and fall onto an outstretched arm, or falling on a shoulder may cause a SLAP tear. • Even bracing oneself, with arms outstretched, in a car accident
Symptoms • catching sensation • pain with shoulder movements, most often overhead activities such as throwing. • pain deep within the shoulder or in the back of the shoulder joint. • It is often hard to pinpoint symptoms, unless the biceps tendon is also involved. In cases of SLAP tears with associated biceps tendonitis, patients may complain of pain over the front of the shoulder
Diagnoses • SLAP tears tend to be seen best on MRI when the study is performed with an injection of contrast.
Anterior Slide Test • involves the arm to be examined is positioned with the hand on the ipsilateral hip with the thumb forward. • The examiner then stabilizes the scapula with one hand and provides an anterosuperiorly directed axial load to the humerus with the other hand. • The test is considered positive if there is a click or deep pain in the shoulder during this maneuver • Sensitivity: 8-78%, Specificity: 84%, PPV: 5%, NPV: 90% (These results are from a combination of many different studies, you can see the large variability)
Biceps Load and Biceps Load II Tests • during this test, the shoulder is placed in 90 degrees of abduction and maximally externally rotated. • At maximal external rotation and with the forearm in a supinated position, the patient is instructed to perform a biceps contraction against resistance. • Deep pain within the shoulder during this contraction is indicative of a SLAP lesion. • The original authors further refined this test with the description of the biceps load II maneuver. The examination technique is similar, although the shoulder is placed into a position of 120 degrees of abduction rather than the originally described 90 degrees. The biceps load II test was noted to have greater sensitivity than the original test. • Sensitivity: 91%, Specificity: 97%, PPV: 83%, NPV: 98% for Biceps Load I; Sensitivity: 90%, Specificity: 97%, PPV: 92%, NPV: 96% for Biceps Load II
Pain Provocation Test • During this maneuver, the shoulder is passively abducted to 90-100 degrees and passively externally rotated with the forearm in full pronation and then full supination. • SLAP lesion was present if pain was produced with shoulder external rotation with the forearm in the pronated position or if the severity of the symptoms was greater in the pronated position. • The authors note that positive symptoms with this test are due to the additional stretch placed on the biceps tendon when the shoulder is externally rotated with the forearm pronated. • Sensitivity: 100%, Specificity: 90%
SLAP tears into three categories • Overhead Athletes that present with peel-back lesions • Compression injuries from someone that falls onto an outstretched arm or on the side of the shoulder. This will compress and sheer the labrum, similar to a meniscus tear. • Traction injuries from a sudden eccentric biceps contraction. This one is the least common and I even have some mild doubts of this mechanism.
Basic types are Type I-IV. • Type I – fraying/degeneration of labrum edge • Type II – defect (fray/degeneration) into the labrum; commonest type; requires surgical repair • Type III - bucket handle tear; uncommon; requires surgical repair • Type IV - bucket handle tear AND biceps tendon tear; uncommon; requires surgical repai
Treatment • Most patients with SLAP tears will respond to conservative (meaning non-surgical) treatments. • Any patient with a SLAP tear will be advised to rest after the injury to allow the injured tissue to cool down. • A period of rest will allow inflammation to subside and may help to alleviate symptoms.
Rehabilitation • The therapy is designed to restore range of motion and strength to the shoulder.
Debridement of the SLAP tear • When a SLAP tear is debrided, the torn portion of the labrum is shaved away to leave a smooth edge. • This option is only suitable for minor tears that do not involve the biceps tendon.
Biceps Tenodesis • procedure that cuts the biceps tendon from where it attaches to the labrum, and reinserts it in another area. • The idea behind a biceps tenodesis is that by decreasing the forces that pull on the SLAP region, the symptoms will be alleviated. • A biceps tenodesis is most often performed on patients over 40 years of age or patients with associated biceps tendonitis or tearing. • A biceps tenodesis can either be performed arthroscopically, or through a small incision over the top of the shoulder.
SLAP repair • A SLAP repair is an arthroscopic procedure that uses sutures with anchors attached to resecure the torn labrum down to the shoulder socket. • A SLAP repair is best suited to patients with an otherwise healthy shoulder who want to remain athletically active.
Advantages of a SLAP repair? • Restores the normal anatomy of the shoulder by reattaching the labrum in its normal position. • Once healed, the SLAP repair allows normal function of the previously damaged labrum and biceps attachment. • What are the advantages of other treatments such as debridement or tenodesis? • The rehabilitation is often not as restrictive as is the case with a SLAP repair. • The results of surgery are usually more predictable, as healing of a SLAP repair is not as reliable.
Rehab after a SLAP repair • Rehabilitation varies depending on factors such as the strength of the SLAP repair, and the preference of the surgeon. • Most often, a period of time of restricted motion is maintained for about six weeks following a SLAP repair. • During this first phase of rehabilitation, some passive motion is allowed to prevent shoulder stiffness. In the first phase, the torn labrum is healing into its proper position. • Once healed, patients enter the second phase of rehabilitation and can begin more motion at about six weeks. • Physical therapy continues to help maintain motion and regain strength of the shoulder. The final phase of rehabilitation involves more active strengthening of the muscles that surround the shoulder joint, and full recovery is expected between 3 to 4 months.
Return to Sports? • 6 months after surgery. You must have good motion, strength, and control of your shoulder and arm. • Overall, the success rate for SLAP repair ranges from 85 to 95%. • The goal is to achieve a shoulder with no pain for throwing or overhead activity.