
ABG
E N D
Presentation Transcript
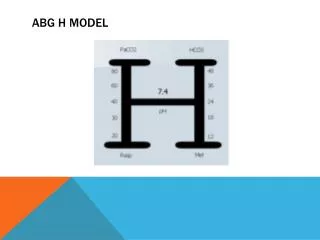
Arterial Blood Gas Interpretation HOSAM M ATEF;MD PART 2 SUEZ CANAL UNIVERSITY
Rules for Respiratory Acid-Base Disorders • Rule 1 : The 1 for 10 Rule for Acute Respiratory Acidosis The [HCO3] will increase by 1 mmol/l for every 10 mmHg elevation in pCO2 above 40 mmHg. • Expected [HCO3] = 24 + { (Actual pCO2 - 40) / 10 }
Rule 2 : The 4 for 10 Rule for Chronic Respiratory Acidosis The [HCO3] will increase by 4 mmol/l for every 10 mmHg elevation in pCO2 above 40mmHg. • Expected [HCO3] = 24 + 4 { (Actual pCO2 - 40) / 10}
Rule 3 :The 2 for 10 Rule for Acute Respiratory Alkalosis The [HCO3] will decrease by 2 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg. • Expected [HCO3] = 24 - 2 { ( 40 - Actual pCO2) / 10 }
Rule 4 : The 5 for 10 Rule for a Chronic Respiratory Alkalosis The [HCO3] will decrease by 5 mmol/l for every 10 mmHg decrease in pCO2 below 40 mmHg. • Expected [HCO3] = 24 - 5 { ( 40 - Actual pCO2 ) / 10 } ( range: +/- 2) • It takes 2 to 3 days to reach maximal renal compensation • The limit of compensation is a [HCO3] of about 12 to 15 mmol/l
Rules for Metabolic Acid-Base Disorders • Rule 5 : The One & a Half plus 8 Rule - for a Metabolic Acidosis The expected pCO2 (in mmHg) is calculated from the following formula: • Expected pCO2 = 1.5 x [HCO3] + 8 (range: +/- 2) • Maximal compensation may take 12-24 hours to reach The limit of compensation is a pCO2 of about 10 mmHg • Hypoxia can increase the amount of peripheral chemoreceptor stimulation
Rule 6 : The Point Seven plus Twenty Rule - for a Metabolic Alkalosis The expected pCO2(in mmHg) is calculated from the following formula: • Expected pCO2 = 0.7 [HCO3] + 20 (range: +/- 5)
Anion Gap Metabolic acidosis is conveniently divided into elevated and normal anion gap (AG) acidosis. AG is calculated as AG = Na+ - (Cl- + CO2)
Note: CO2 in this equation is the “total CO2”consists mostly of bicarbonate. • Normal AG is typically 12 ± 4 mEq/L. If AG is calculated using K+, the normal AG is 16 ± 4 mEq/L. • Normal values for AG may vary among labs, so one should always refer to local normal values before making clinical decisions based on the AG.
Differential diagnosis of metabolic acidosis 13 13 HCO3 HCO3 HCO3 25 Na 140 Na 140 Na 140 CL CL 103 115 103 CL 24 A- 12 A- A- 12 Normal A- High A- Normal acidosis acidosis A- = anion gap
High anion gap Normal anion gap Diarrhea/fistula/ileal loopRTADiamox Early renal failure Hyperparathyroidism Ketoacidosis Uremia Lactic acidosis Toxins: Ethylene glycol methanol paraldehyde salicylate
NaHCO3 • Normal anion gap pH < 7.1 ( HCO3 < 15) • Hypotension refractory to volume and inotropic support 1/3 wt × base deficit 50 % - recheck When to use How to use
NaHCO3 Molar solution= 23 +1+12+48 = 84 g/l ( 8.4 % solution) Molar solution = 84 g/l ( 8.4 % ) = 84 g/1000 ml = 1 mol/1000 ml = 1000 mmol/1000 ml = 1 mmol/ml
Differential diagnosis of metabolic alkalosis Chloride responsive Chloride resistant ( loss of chloride ) ( loss of H+ ) vomiting diarrhea Mg K diuretics aldos < 20 > 20 Urine chloride ( mmol/L)
Treatment of metabolic alkalosis Chloride resistant • Na Cl = 30% × Bwt × ( 100 - Clm) • HCl = 50% × Bw × BE • Drugs Acetazolamide H2 blockers Chloride responsive • Aldosterone antagonists • K • Mg
Anion gap (measured)-Anion gap (normol)Hco3(normol)-Hco3(measured) DELTA RATIO
High anion gap HCO3 gap = Na-Cl-36 < - 6 > 6 Associated normal AG acidosis Associated metabolic alkalosis
Osmgap ΔOsmgap = Osmmeasured − Osmcalculated(mOsm/kg). The measured osmolality 285 and 295 mOsm/kg The normal osmolal gap is <10 to 12 mOsm/kg H2O.
SIG approach SSIDa = Na + K+ Ca+ Mg- (Cl+lactate) IDa= Na + K+ Ca+ Mg- (Cl+lactate) Na K Ca Mg HCO3 SIDe Alb. SIDe = HCO3 + 0.28 * Albumin (g/L) + 1.8 * Pi (mmol/L) P XA Cl SIG= SIDa- SIDe the “normal” SIG as 8 ± 2 mEq/L (Fencl et al., 2000)
Metabolic Acid-Base Disorders -- Some clinical causes -- METABOLIC ACIDOSISIncreased anion gap • lactic acidosis; ketoacidosis; drug poisonings (e.g., aspirin, ethyelene glycol, methanol) • Normal anion gap • diarrhea; some kidney problems, e.g., renal tubular acidosis, intersititial nephritis
Respiratory Acid-Base Disorders -- Some clinical causes -- RESPIRATORY ACIDOSIS Central nervous system depression (e.g., drug overdose) Chest bellows dysfunction (e.g., Guillain-Barré syndrome, myasthenia gravis) Disease of lungs and/or upper airway (e.g., chronic obstructive lung disease, severe asthma attack, severe pulmonary edema)
RESPIRATORY ALKALOSIS Hypoxemia (includes altitude) Anxiety Sepsis Any acute pulmonary insult, e.g., pneumonia, mild asthma attack, early pulmonary edema, pulmonary embolism
METABOLIC ALKALOSIS Chloride responsive (responds to NaCl or KCl therapy): contraction alkalosis, diuretics; corticosteroids; gastric suctioning; vomiting • Chloride resistant: any hyperaldosterone state, e.g., Cushings’s syndrome; Bartter’s syndrome; severe K+ depletion
Mixed Acid-base disorders are common • In chronically ill respiratory patients, mixed disorders are probably more common than single disorders, e.g., RAc + MAlk, RAc + Mac, Ralk + MAlk. • In renal failure (and other patients) combined MAlk + MAc is also encountered. • Always be on lookout for mixed acid-base disorders. They can be missed!
Tips to diagnosing mixed acid-base disorders TIP 1. Don’t interpret any blood gas data for acid-base diagnosis without closely examining the serum electrolytes: Na+, K+, Cl- and CO2. • Note that serum CO2 may be normal in the presence of two or more acid-base disorders.
Tips to diagnosing mixed acid-base disorders (cont.) TIP 2. a truly normal pH with distinctly abnormal HCO3- and PaCO2 invariably suggests two or more primary disorders. • Example: pH 7.40, PaCO2 20 mm Hg, HCO3- 12 mEq/L, in a patient with sepsis. Normal pH results from two co-existing and unstable acid-base disorders: acute respiratory alkalosis and metabolic acidosis.
Tips to diagnosing mixed acid-base disorders (cont.) TIP 3. Simplified rules predict the pH and HCO3- for a given change in PaCO2. If the pH or HCO3- is higher or lower than expected for the change in PaCO2, the patient probably has a metabolic acid-base disorder as well.
Predicted changes in HCO3- for a directional change in PaCO2 can help uncover mixed acid-base disorders. a) A normal or slightly low HCO3- in the presence of hypercapnia suggests a concomitant metabolic acidosis, e.g., pH 7.27, PaCO2 50 mm Hg, HCO3- 22 mEq/L. Based on the rule for increase in HCO3- with hypercapnia, it should be at least 25 mEq/L in this example; that it is only 22 mEq/L suggests a concomitant metabolic acidosis.
Predicted changes in HCO3- for a directional change in PaCO2 can help uncover mixed acid-base disorders. b) A normal or slightly elevated HCO3- in the presence of hypocapnia suggests a concomitant metabolic alkalosis, e.g., pH 7.56, PaCO2 30 mm Hg, HCO3- 26 mEq/L. Based on the rule for decrease in HCO3 with hypocapnia, it should be at least 23 mEq/L in this example; that it is 26 mEq/L suggests a concomitant metabolic alkalosis
Tips to diagnosing mixed acid-base disorders (cont.) TIP 4. In maximally-compensated metabolic acidosis, the numerical value of PaCO2 should be the same (or close to) the last two digits of arterial pH. This observation reflects the formula for expected respiratory compensation in metabolic acidosis: Expected PaCO2 = [1.5 x serum CO2] + (8 ± 2)
Acid-base disorders 1. A patient’s arterial blood gas shows pH of 7.14, PaCO2 of 70 mm Hg, and HCO3- of 23 mEq/L. How would you describe the likely acid-base disorder(s)? 2. A 45-year-old man comes to hospital complaining of dyspnea for three days. Arterial blood gas reveals pH 7.35, PaCO2 60 mm Hg, PaO2 57 mm Hg, HCO3- 31 mEq/L. How would you characterize his acid-base status?
Acid-base disorders 1. an acute respiratory acidosis. For every 10 mm Hg rise in PaCO2 (before any renal compensation), pH falls about 0.07 units. Because this patient's pH is down 0.26 more than expected for a 30 mm Hg increase in PaCO2, there must be an additional, metabolic problem. Also, note that with acute CO2 retention of this degree, the HCO3- should be elevated 3 mEq/L. Thus a low-normal HCO3- with increased PaCO2 is another way to uncover an additional, metabolic disorder. Decreased perfusion leading to mild lactic acidosis would explain the metabolic component.
Acid-base disorders • 2. PaCO2 and HCO3- are elevated, but HCO3- is elevated more than would be expected from acute respiratory acidosis. Since the patient has been dyspneic for several days( a chronic acid-base disorder). Most likely this patient has a chronic or partially compensated respiratory acidosis. Without electrolyte data and more history, you cannot diagnose an accompanying metabolic disorder.
Acid-base disorders 3. State whether each of the following statements is true or false. a) Metabolic acidosis is always present when the measured serum CO2 changes acutely from 24 to 21 mEq/L.F b) In acute respiratory acidosis, bicarbonate initially rises because of the reaction of CO2 with water and the resultant formation of H2CO3.T c) If pH and PaCO2 are both above normal, the calculated bicarbonate must also be above normal.T d) An abnormal serum CO2 value always indicates an acid-base disorder of some type.T e) The compensation for chronic elevation of PaCO2 is renal excretion of bicarbonate.F f) A normal pH with abnormal HCO3- or PaCO2 suggests the presence of two or more acid-base disorders.T g) A normal serum CO2 value indicates there is no acid-base disorder.F
Arterial Blood Gases • Case 1. A 55-year-old man is evaluated in the pulmonary lab for shortness of breath. His regular medications include a diuretic for hypertension and one aspirin a day. He smokes a pack of cigarettes a day. • FIO2 .21 HCO3- 30 mEq/L • pH 7.53 %COHb 7.8% • PaCO2 37 mm Hg Hb 14 gm% • PaO2 62 mm Hg CaO2 16.5 ml O2 • SaO2 87% • How would you characterize his state of oxygenation, ventilation and acid-base balance?
Arterial Blood Gases Case 1 - Discussion. OXYGENATION: The PaO2 and SaO2 are both reduced on room air. Since P(A-a)O2 is elevated (approximately 43 mm Hg), the low PaO2 can be attributed to V-Q imbalance, i.e., a pulmonary problem. SaO2 is reduced, in part from the low PaO2 but mainly from elevated carboxyhemoglobin, which in turn can be attributed to cigarettes. The arterial oxygen content is adequate. VENTILATION: Adequate for the patient's level of CO2 production; the patient is neither hyper- nor hypo- ventilating. ACID-BASE: Elevated pH and HCO3- suggest a state of metabolic alkalosis, most likely related to the patient's diuretic; his serum K+ should be checked for hypokalemia.
Arterial Blood Gases – test your overall understanding • Case 2. A 46-year-old man has been in the hospital two days, with pneumonia. He was recovering but has just become diaphoretic, dyspneic and hypotensive. He is breathing oxygen through a nasal cannula at 3 l/min. • pH 7.40 • PaCO2 20 mm Hg • %COHb 1.0% • PaO2 80 mm Hg • SaO2 95% • Hb 13.3 gm% • HCO3- 12 mEq/L • CaO2 17.2 ml O2 • How would you characterize his state of oxygenation, ventilation and acid-base balance?
Arterial Blood Gases Case 2 - Discussion. OXYGENATION: The PaO2 is lower than expected for someone hyperventilating to this degree and receiving supplemental oxygen, and points to significant V-Q imbalance. The oxygen content is adequate. VENTILATION: PaCO2 is half normal and indicates marked hyperventilation. ACID-BASE: Normal pH with very low bicarbonate and PaCO2 indicates combined respiratory alkalosis and metabolic acidosis. If these changes are of sudden onset the diagnosis of sepsis should be strongly considered, especially in someone with a documented infection.