ABG
ABG. APPROACH TO INTERPRETATION OF ABG. Know the primary disorder Compute for the range of compensation For metabolic acidosis get anion gap For high anion gap get change in anion gap and compare with change in bicarbonate. COMPENSATORY RESPONSE. COMPENSATORY RESPONSES. Case 1.

ABG
E N D
Presentation Transcript
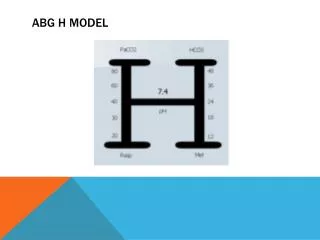
APPROACH TO INTERPRETATION OF ABG • Know the primary disorder • Compute for the range of compensation • For metabolic acidosis get anion gap • For high anion gap get change in anion gap and compare with change in bicarbonate
Case 1 • A 55 year-old female, a known diabetic for 10 years, came in at the ER for a 3 day history of fever and productive cough with anasarca, abdominal pain and vomiting • Labs: • RBS – 22 (396) • BUN – 3.6 • Crea- 323 mmol/L • Ca – 1.88 • Alb – 22 • Urine ketone +++ • Na - 129 • K – 3.8 • Cl – 98 • Phos – 3.2 • USG – 1.030 ABG: pH – 7.135 pCO2 – 20.2 pO2 – 89 HCO3 – 12.4 BE – -9.0 O2 sats – 98%
Case 1 ABG: pH – 7.135 pCO2 – 20.2 pO2 – 89 HCO3 – 12.4 BE – -9.0 O2 sats – 98% Room air • Interpret ABG • Look at the pH • Acidotic • What caused the pH • Metabolic acidosis • Compute for compensation • Decrease in pCO2 = 1.2 x change in bicarbonate • Expected pCO2: • Expected pCO2 = 26 • Expected pCO2 is higher than actual pCO2 (20.2), therefore there is concomitant respiratory alkalosis
Case 1: • Interpret ABG • If metabolic, compute the anion gap • Get the corrected Na: • Corrected Na = (RBS – 100) x 0.016 + Na • Corrected Na = 134 • Compute the anion gap: • Anion gap = Na – HCO3 – Cl • Anion gap = 23.6 • HAGMA
Case 1: • Interpret ABG • Get delta-delta: • Change in anion gap • Change = AG - 12 • Change = 11.6 • Change in bicarbonate • Change = 24 – bicarbonate • Change = 11.6 • Change in AG = change in bicarbonate • Therefore: pure HAGMA • Otherwise: • Change in AG > change in bicarbonate: HAGMA + metab alkalosis • Change in AG < change in bicarbonate: HAGMA + NAGMA
Case 1: ABG: pH – 7.135 pCO2 – 20.2 pO2 – 89 HCO3 – 12.4 BE – -9.0 O2 sats – 98% Room air • Interpret ABG • Check for pO2 • Correlate with FiO2 • LPM to FiO2 at nasal cannula: 4 x LPM + 20 • Hypoxemia (pO2 at FiO2 21%) • Mild: 80-90 • Moderate: 60-80 • Severe: < 60
Case 1: • Final ABG interpretation: • High anion gap metabolic acidosis with concomitant respiratory alkalosis, mild hypoxemia
Case 1: • Conditions that lead to metabolic acidosis: • HAGMA • DKA • Alcoholic ketoacidosis • Lactic acidosis • Renal insufficiency • Starvation • Salicylate intoxication • Methanol intoxication • Ethylene glycol intoxication • NAGMA • Diarrhea • Pancreatic fluid loss • Ileostomy • Carbonic anhydrase inhibitors • RTA • Arginine and lysine in parenteral nutrition
Case 2: • Case 2: A 55 year-old female, a known diabetic for 10 years came in at the ER for a 3-day history of fever and productive cough with anasarca, abdominal pain and vomiting • RBS – 22 • BUN – 13.2 • Crea – 323 • Ca – 1.62 • Alb – 22 • Urine ketone + • Na – 117 • K – 2.8 • Cl – 98 • Phos – 6.2 • USG – 1.025 ABG: pH – 7.535 pCO2 – 45.22 pO2 – 89.00 HCO3 – 30.40 BE – 6.0 O2 sats – 98%
Case 2: ABG: pH – 7.535 pCO2 – 45.22 pO2 – 89.00 HCO3 – 30.40 BE – 6.0 O2 sats – 98% 10 lpm • Interpret ABG • Look at the pH • Alkalotic • What caused the pH • Metabolic alkalosis • Compute for compensation • increase in pCO2 = 0.7 x change in bicarbonate • Expected pCO2: • Expected pCO2 = 44.48 • Expected PCO2 is near actual pCO2. Therefore, patient has compensated metabolic alkalosis
Case 2: ABG: pH – 7.535 pCO2 – 45.22 pO2 – 89.00 HCO3 – 30.40 BE – 6.0 O2 sats – 98% 10 lpm • Interpret ABG • Check for pO2 • Correlate with FiO2 • LPM to FiO2 at nasal cannula: 4 x LPM + 20 • Hypoxemia (pO2 at FiO2 21%) • At FiO2 21%, pO2 should be at least 90 • Target pO2 = 90 / 0.21 x FiO2 • Target pO2 - 257 • hypoxemia
Case 2 • Final ABG interpretation: • Compensated metabolic alkalosis, with hypoxemia
Case 2: • Conditions associated with metabolic alkalosis: • Diuretic therapy • Posthypercapnia • Vomiting • Nasogastric suction • NaHCO3 • Refeeding alkalosis • Primary aldosteronism • Hyperreninism • Liddle’s syndrome • Licorice (exogenous mineralocorticoids)
Case 3: • A 50 year old male, with a 50 pack year smoking history presents at the ER for chronic cough, weight loss, with a 3 day history of high-grade fever and dyspnea for which he took cotrimoxazole 800/160 mg TID. Early this morning, he was found unresponsive and was then brought to the ER. On PE, there was note of tachypnea, poor air entry and ocassional wheezing all over • RBS – 6.3 • BUN – 8.3 • Crea- 96 • Ca – 1.92 • Alb – 22 • USG – 1.035 • Na – 163 • K – 7.8 • Cl – 98 • Phos – 4.6 • 12L ECG – ST, NA, NSSTWCs ABG: pH – 7.135 pCO2 – 70.2 pO2 – 49.00 HCO3 – 24.20 BE – -2.0 O2 sats – 78%
Case 3: • Interpret ABG • Look at the pH • acidotic • What caused the pH • Respiratory acidosis • Compute for compensation • increase in HCO3 = 1/10 x change in pCO2 (acute) • Increase in HCO3 = 3/10 x change in pCO2 (chronic) • Expected HCO3: (acute) • Expected HCO3 = 27 • Expected HCO3 is higher than actual HCO3 (24.20). Therefore, patient has uncompensated respiratory acidosis ABG: pH – 7.135 pCO2 – 70.2 pO2 – 49.00 HCO3 – 24.20 BE – -2.0 O2 sats – 78% 5 LPM
Case 3: ABG: pH – 7.135 pCO2 – 70.2 pO2 – 49.00 HCO3 – 24.20 BE – -2.0 O2 sats – 78% 5 LPM • Interpret ABG • Check for pO2 • Correlate with FiO2 • LPM to FiO2 at nasal cannula: 4 x LPM + 20 • Hypoxemia (pO2 at FiO2 21%) • Expected pO2 = 90/0.21 x FiO2 • Expected pO2 = 171 • hypoxemia
Case 3 • Final ABG interpretation: • Uncompensated respiratory acidosis with hypoxemia
Case 3 • Conditions associated respiratory acidosis: • Airway obstruction • Respiratory center depression • Neuromuscular defects • Restrictive defect
Case 4: • A 50 year old male, with a 50 pack-year smoking history presents at the ER for chronic cough, weight loss, with 3 day history of low grade fever and dyspnea for which he took cotrimoxazole 800/160 mg TID. Early this morning, he was found unresponsive and was then brought to the ER. On PE, there was note of tachypnea, poor air entry and occasional wheezing all over • RBS – 6.3 • BUN – 14.3 • Crea – 96 • Ca - 2.42 • Alb – 22 • USG – 1.015 • Na – 113 • K – 7.8 • Cl – 98 • Phos – 4.6 • 12L ECG – ST, NA, shortened Qt, peaked T waves ABG: pH – 7.48 pCO2 – 30.2 pO2 – 49.00 HCO3 – 25.50 BE – -1.8 O2 sats – 78%
Case 4: ABG: pH – 7.48 pCO2 – 30.2 pO2 – 49.00 HCO3 – 25.50 BE – -1.8 O2 sats – 78% 6 LPM • Interpret ABG • Look at the pH • alkalosis • What caused the pH • Respiratory alkalosis • Compute for compensation • decrease in HCO3 = 2/10 x change in pCO2 (acute) • decrease in HCO3 = 5/10 x change in pCO2 (chronic) • Expected HCO3: (acute) • Expected HCO3 = 22.04 • Expected HCO3 is lower than actual HCO3 (25.50). Therefore, patient has concomitant metabolic alkalosis
Case 4: ABG: pH – 7.48 pCO2 – 30.2 pO2 – 49.00 HCO3 – 25.50 BE – -1.8 O2 sats – 78% 6 LPM • Interpret ABG • Check for pO2 • Correlate with FiO2 • LPM to FiO2 at nasal cannula: 4 x LPM + 20 • Hypoxemia (pO2 at FiO2 21%) • Target pO2 = 90/0.21 x FiO2 • Target pO2 = 189 • hypoxemia
Case 4: • Final ABG interpretation: • Respiratory alkalosis with concomitant metabolic alkalosis
Case 4: • Conditions associated with respiratory alkalosis: • High altitude • V/Q mismatch • Severe anemia • Infection • trauma • Hepatic failure • Gram negative septicemia • Interstitial lung disease • Pneumonia • Pulmonary embolism • Pulmonary edema