Download
1 / 21
210 likes | 552 Vues
Improving Interconception Care for High Risk Women. February 10, 2011 Low Country Healthy Start “Every Woman Southeast Initiative” Webinar. Virginia Berry White, LMSW vbwhite@lchealthystart.org. Interconception Care – Learning Community – MCHB, HRSA, Healthy Start Program.

E N D
Improving Interconception Care for High Risk Women February 10, 2011 Low Country Healthy Start “Every Woman Southeast Initiative” Webinar Virginia Berry White, LMSW vbwhite@lchealthystart.org
Interconception Care – Learning Community – MCHB, HRSA, Healthy Start Program Improve Health and Well-Being of Women Advance Quality & Effectiveness of Interconception Care Implementation of Evidenced-Based Practices Innovative Community-Driven Interventions Home Team and Traveling Team (Learning Sessions) Expert Work Group Abt Associates, Inc. and Johnson Group Consulting, Inc. 2
Interconception Care – Learning Community – MCHB, HRSA, Healthy Start Program All Healthy Start Programs are required to participate CQI Process, using Plan, Do, Study, Act principles Choices of Major Focus Area include: Family Planning & Reproductive Health Primary Care Services & Linkages Maternal Depression & Mental Health Healthy Weight Risk Screening Low Country Healthy Start (LCHS) chose Family Planning and Reproductive Health – strongly linked with working with primary care providers 3
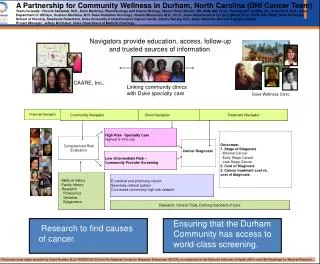
Route to Get to: • Strengthening partnerships and linkages among providers • Taking evidenced-based protocols and implementing • Improving staff training and protocols to improve quality and consistency HS ICC-LC
To get to improvements and outcomes is not a fast process; a long road to travel.
About LCHS • Part of the SC Office of Rural Health • Service area is four rural counties in the Low Country region of the state • Allendale, Bamberg, Hampton and Orangeburg • Six (6) sites • LCHS is staffed by masters prepared social workers and lay home visitors, called Client Navigators • Home Visiting, Case Management, social work, outreach and coordination program • Target population is African American women
Description of Project Area • Very poor, under-resourced counties • Birthing Hospital in only one of four counties • High unemployment rates • In 2008, there were 1,385 African American live births in the service area, 592 white births and 23 other • In 2010, LCHS provided services to 1, 449 families - 380 pregnant women, 409 postpartum women and 660 infants • LCHS program criteria, woman at risk for poor pregnancy outcomes and her newborn • Reduce the rate of Infant Mortality • Eliminate disparities in perinatal health
Barriers (serving High Risk Women) • Lack of insurance coverage • Women not knowing services that are available, i.e., Family Planning Waiver • Access to care • Woman’s access to contraceptives of her choice • Psychosocial and economic issues • Client retention during the interconception (postpartum) period • Coordination of care • Shortage of providers
Barriers (serving High Risk Women) • Patient-Provider Communication/Relationship • Time allotted to counsel women during office visits • Inability for providers to pay for long-term methods • Few obstetric and prenatal providers • Women understanding of what is required to increase her chances of having a healthy baby • Women inability to secure access to risk appropriate care • Health of Women of Childbearing Age
LCHS Interconception Care, Family Planning & Reproductive Health Increase the percent of intended pregnancies ▫Address Barriers ▫Partnership with Provider and LCHS program participants Decrease unintended pregnancy ▫Family Planning Options/Link to FP Services ▫Pregnancy Spacing ▫Survey Family Planning Providers Decrease late prenatal care Decrease poor pregnancy outcomes when women do not intend to be pregnant 12
Model: Use of Multidisciplinary Teams (MDT) for Addressing Interconception Care for High Risk Women Partners Private obstetric practices Monthly Meetings Forge closer connection between LCHS and the perinatal providers Specific client centered discussions aid in learning and teaching, as well as joint care planning MDT learn from LCHS more about the client’s home situation and home/life stress LCHS staff learn more about the clinical side of prenatal, postpartum and interconception care 13
Successes/LCHS and Providers“Voice of the Providers” Certified Nurse Midwives involving Obstetricians Tie LCHS work, Interconceptional Focus into Prematurity Prevention (begins before next pregnancy) Insight gained into the needs of women Centering Pregnancy – prenatal & postpartum periods Home visits are key, esp. to high risk women with subsequent pregnancies Find ways to provide family planning services to indigent clients Standing order through birthing hospital (women will leave the hospital with a method) 14
Data System Client’s Reproductive & Interconception Health begin at prenatal Risk Assessment Automated trigger reminders – LCHS Data System Reminder about EDC & delivery date, Family Planning option, Postpartum exam Automated edit reports – LCHS Data System - Specific information missing from client’s file - Examples: Did she leave hospital after delivery with a method? What is the postpartum visit date? Did she go? Birth control method selected? Did she receive? Tracking client by method selected and follow-up dates by type of method. 15
Implementing Changes - Steps • LCHS staff were trained on the importance of women understanding birth control methods, trained on the effectiveness and risks of each and trained to discuss methods with women, helping them choose • LCHS staff were trained on program expectations of when in the prenatal period BC methods will be discussed, how to document, the expectations for close follow-up and documentation in the two years after delivery • Data collection tools and logs were discussed, along with responsibility for completion • Data are collected, results analyzed and shared with the PPAG and Home Team.
Success to Date • LCHS developed a tracking log used by staff to collect and report data on each client after she delivers. • Improvements have been documented in the number of women leaving the birthing hospital in the service area with Depo Provera (or a permanent method such as tubal ligation or hysterectomy). • Results and progress are reported to partners, the Perinatal Provider Advisory Group, MDT members and LCHS Staff. • The PPAG and MDT partners are consulted about the strategy, implementation success and are frequently asked for additional input.
Success to Date • Providers are now openly discussing what has to be done to help women gain access to effective long-lasting contraceptives, particularly the Mirena IUD. • LCHS has met with the SC Primary Care Association, who then agreed to form a study group, to determine how the FQHCs can overcome perceived barriers to providing long acting, effective birth control methods for clients. • LCHS has met with physicians and NP representing all FQHCs in the service area to identify problems and find solutions.
Measuring Change • # of partners (delivering providers) using the protocol to assure women are discharged from the hospital, after delivery, with a method. LCHS will partner with 4; 1 per county. # of primary care partners accepting our referrals and assisting clients to select and use an effective contraceptive method. Planned number is 8; 2 per county. Assisting clients with selecting and using an effective contraceptive method is defined as LCHS or the client securing an appointment within 2 weeks of appointment request. Payment for care is not a barrier which means the client has Medicaid, other insurance and/or the provider has agreed to accept LCHS referrals for free, or low cost or uses a sliding fee scale . • # of LCHS post-partum clients using a birth control method effectively at 3, 6, 9, 12, 18, 24 months. Target is 75%.
Where do we plan to go from here? • Improve data collection and data quality. Make data collection more seamless, clarify what is needed and why. Make data fit with data staff already report. • Continue to work with the FQHCs and assure they work with women, prescribe the method women want and then provide the method. • Work with Title V to determine what can be done to improve access to Title X required services given the county health department staffing issues. Propose Title X sub-contract to other providers for services they cannot provide adequately, appropriately or timely. • Continue to work with the birthing hospital and obstetric providers to keep the focus on interconception care. • Work with other hospitals, outside the service area, to use the protocol. • Continue to find (and implement) even more effective ways to help women advocate for their own reproductive health desires, requirements and needs.
Low Country Healthy Start Post Office Box 2889 Orangeburg, SC 29116 803-531-8008 803-531-8007 – Fax Virginia Berry White, LMSW vbwhite@lchealthystart.org