The Aphasias
The Aphasias. Woodford A. Beach, MS, CCC/SP Senior Speech-Language Pathologist Clinical Instructor, Otolaryngology MCVH&P of VCUHS May 3, 2002. Objectives. Define aphasia Review Boston aphasia classification Consider atypical aphasias Note other neurogenic communication disorders.

The Aphasias
E N D
Presentation Transcript
The Aphasias Woodford A. Beach, MS, CCC/SP Senior Speech-Language Pathologist Clinical Instructor, Otolaryngology MCVH&P of VCUHS May 3, 2002
Objectives • Define aphasia • Review Boston aphasia classification • Consider atypical aphasias • Note other neurogenic communication disorders
Aphasia • acquired language disorder, that is a CNS disturbance of the capacity to interpret and formulate symbols for communicative purposes • secondary to focal brain damage • perisylvian region • dominant hemisphere • not due to diffuse or multifocal dysfunction
Aphasia • characterized by impairment in connected speech and conversation, auditory comprehension, repetition, naming, reading, & writing
Dysarthria • group of speech disorders • neurogenic • associated with CNS, PNS, muscle pathology
Dysarthria • movement disorder • abnormal neuromuscular execution • affects speed, strength, timing, accuracy • affects respiration, phonation, resonance, articulation, and prosody Darley, Aronson, & Brown 1975
Apraxia of Speech • disorder of motor planning • absence of aphasia & neuromotor deficits • characterized by symptom variability • mutism • difficulty initiating speech • problems in syllable transition • more difficulty in volitional than automatic • more difficulty in long than short • more difficulty in complex than simple
Apraxia of Speech • Often • articulatory struggle • phoneme metathesis • syllable transposition Duffy 1995
Aphasia is not language of confusion • Aphasia is not due to psychiatric disease • Aphasia is not due to primary cognitive dysfunction • it is focal, and not caused by multifocal or diffuse brain disease
Assessment of Aphasia:Formal • Boston Diagnostic Aphasia Examination • Western Aphasia Battery • Burns Left Hemisphere Inventory • Boston Assessment of Severe Aphasia • Aphasia Diagnostic Profiles • Boston Naming Test • Minnesota Test for the Differential Diagnosis of Aphasia
Assessment of Aphasia:Informal • Conversation & Connected Speech • fluent • hyperfluent (logorrhea or press of speech) • nonfluent • grammatic/paragrammatic/agrammatic • empty • appropriate without dyspragmias
Assessment of Aphasia:Informal • Conversation & Connected Speech • if there is only minimal speech • automatic series (counting, days of week) • singing • does the patient engage linguistically
Assessment of Aphasia:Informal • Auditory Comprehension • commands • 1 part axial • 1 part other • 2 part • 3 part • yes/no questions with known answer • orientation • bizarre • complex
Assessment of Aphasia:Informal • Repetition • repeat sentences • “No ifs, ands, or buts” • “They heard him speak on the radio last night” • repeat words • vary length and familiarity
Assessment of Aphasia:Informal • Word Retrieval • confrontation • name objects • name parts of objects • responsive • answer questions • verbal fluency • list words belonging to semantic class or beginning with common letter
Assessment of Aphasia:Informal • Word Retrieval Errors • paraphasias: word substitutions • circumlocutions: talk around target • neologisms: nonwords • stereotypy: restricted subpropositional forms (often yes & no) • frank dysnomia: no response or do not know
Assessment of Aphasia:Informal • Reading Comprehension • silent reading of command • silent reading of yes/no question • oral reading is not reading comprehension any more than dictation or copying are written expression • If reading comprehension compromised, assess oral reading
Assessment of Aphasia:Informal • Written Expression • generate sentence given stimulus word • automatic writing (e.g. signature) is not written expression • If writing impaired, assess taking dictation, then copying of words or figures
Boston Aphasia Classification • Relative sparing vs relative impairment • Reading and writing always impaired • Differentiate aphasias in • fluency • auditory comprehension • repetition • naming
Nonfluent Broca Global Transcortical Motor Mixed Transcortical (isolation syndrome) Fluent Wernicke Conduction Anomic Transcortical sensory Classic Boston Aphaisas
Disclaimers & caveats re: aphasia taxonomy • Receptive/expressive dichotomy invalid • all aphasias have an expressive component • all aphasias have a receptive component • If you are binary, use the fluent/nonfluent dichotomy
Disclaimers & caveats re: aphasia taxonomy • Other taxonomies exist • Some researchers argue that aphasia is a unary phenomenon • Metter showed that PET scans demonstrate metabolic hypodensities distal to site of lesion (is this diaschisis of von Monokow?) • Reliability dogs all taxonomies
Disclaimers & caveats re: aphasia taxonomy • Taxonomies often fail to capture characterististics of aphasia which are important therapeutically • e.g., Broca’s Aphasia • agrammatism • dysfluency • Labels are abbreviations. Describe Sxs!
Disclaimers & caveats re: aphasia taxonomy • Boston model fails to capture • natural course and evolution of aphasia • severity • localization consistently • Boston group admits: • “In many instances (30-40% of unselected cases), inspection of the speech characteristics leads directly to a diagnostic assignment” Albert et al. 1981 • Therefore, are 60-70% aphasias mixed?
Disclaimers & caveats re: aphasia taxonomy • Research by Nina Dronkers (2000) • Chronic Broca’s • N=12 with Broca’s aphasia • 2 had lesions sparing Broca’s area • 10 others with Broca’s lesion had no persisting Broca’s aphasia • Chronic Broca’s Aphasia always involved insula • Chronic Wernicke’s • N= 7 with Wernicke’s aphasia • 2 had lesions sparing Wernicke’s • 7 others with Wernicke’s lesion had no persisting Wernicke’s aphasia • Chronic Wernicke’s always has large temporal lesion with destruction of posterior MTG • Data reflect structural lesions in chronic aphasias
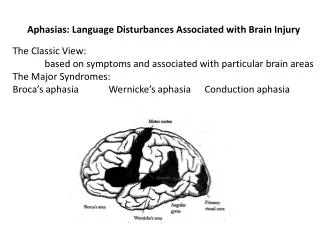
Localization of Classical Aphasias • Broca: third left frontal convolution • Global: entire perisylvian region • Transcortical Motor: anterior watershed • Mixed Transcortical: anterior watershed & posterior watershed
Localization of Classical Aphasias • Broca: third left frontal convolution • Global: entire perisylvian region • Transcortical Motor: anterior watershed • Mixed Transcortical: anterior watershed & posterior watershed
Localization of Classical Aphasias • Broca: third left frontal convolution • Global: entire perisylvian region • Transcortical Motor: anterior watershed • Mixed Transcortical: anterior watershed & posterior watershed
Localization of Classical Aphasias • Broca: third left frontal convolution • Global: entire perisylvian region • Transcortical Motor: anterior watershed • Mixed Transcortical: anterior watershed & posterior watershed
Localization of Classical Aphasias • Wernicke: posterior, superior temporal lobe • Conduction: archuate fasciculus; inferior parietal lobe • Transcortical sensory: posterior watershed • Anomic: posterior: temporoparietal?
Localization of Classical Aphasias • Wernicke: posterior, superior temporal lobe • Conduction: archuate fasciculus; inferior parietal lobe • Transcortical sensory: posterior watershed • Anomic: posterior: temporoparietal?
Localization of Classical Aphasias • Wernicke: posterior, superior temporal lobe • Conduction: archuate fasciculus; inferior parietal lobe • Transcortical sensory: posterior watershed • Anomic: posterior: temporoparietal?
Localization of Classical Aphasias • Wernicke: posterior, superior temporal lobe • Conduction: archuate fasciculus; inferior parietal lobe • Transcortical sensory: posterior watershed • Anomic: posterior: temporoparietal?
Dorsolateral Syndrome • Reduced selective attention • lack of drive & awareness • reduced initiation • dynamic aphasia of Luria • Localize to frontal dorsolateral cortex • anterior and inferior to Broca’s area Frattali 2000