Download
1 / 9
90 likes | 224 Vues
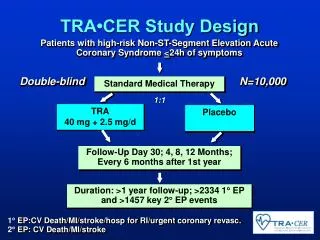
TRA•CER Study Design. Patients with high-risk Non-ST-Segment Elevation Acute Coronary Syndrome < 24h of symptoms. Double-blind. N=10,000. Standard Medical Therapy. 1:1. TRA 40 mg + 2.5 mg/d. Placebo. Follow-Up Day 30; 4, 8, 12 Months; Every 6 months after 1st year.

E N D
TRA•CER Study Design Patients with high-risk Non-ST-Segment Elevation Acute Coronary Syndrome <24h of symptoms Double-blind N=10,000 Standard Medical Therapy 1:1 TRA 40 mg + 2.5 mg/d Placebo Follow-Up Day 30; 4, 8, 12 Months; Every 6 months after 1st year Duration: >1 year follow-up; >2334 1 EP and >1457 key 2 EP events 1EP:CV Death/MI/stroke/hosp for RI/urgent coronary revasc. 2EP: CV Death/MI/stroke
TRA Program TRA Program 29,500 patients Placebo Placebo SCH530348 SCH530348 F/U: 30 Days, 4, 8, 12 months and 6 months thereafter 1 yr minimum, event driven Primary EP: Composite of CV Death, MI, Stroke and Urgent Revascularization Primary EP: Composite of CV Death, MI, Stroke, Recurrent Ischemia with Rehosp, Urgent Coronary Revascularization
5–9 15–19 25–29 35–39 45–49 55–59 65–69 75–79 85–89 >95 <5 10–14 20–24 30–34 40–44 50–54 60–64 70–74 80–84 90–94 Age Distribution of People With AFCompared With U.S. General Population Population with Atrial Fibrillation 500 30,000 400 U.S. Population 20,000 300 AF Population (x 10) U.S. Population (x 1000) 200 10.000 100 0 0 Age (years) Arch Int Med. 1995;155:471.
Warfarin for Atrial FibrillationLimitations Lead to Under-treatment 55% Overall Use 61% 58% 57% 44% Warfarin Use inEligible Patients (%) 35% <55 55-64 65-74 75-84 85 Age (years) Go A et al. Ann Intern Med 1999;131:927.
WarfarinBattling All Comers for Over a Decade • Warfarin vs placebo • Warfarin vs ASA • Warfarin vs ASA + fixed dose wafarin • Warfarin vs DTI • Warfarin vs dual antiplatelet
RELYDabigatran for stroke prevention in atrial fibrillation Non-valvular atrial fibrillation at moderate to high risk of stroke or systemic embolism (at least one high risk factor) R Dabigatran Etexilate 150 mg b.i.d. N=6000 Warfarin 1 mg, 3mg, 5 mg (INR 2.0-3.0) N=6000 Dabigatran Etexilate 110 mg b.i.d. N=6000 • Primary objective: Noninferiority to warfarin • Minimum 1 year follow-up, maximum of 3 years and mean of 2 years of follow-up. • Primary end point: Stroke + systemic embolism
Atrial Fibrillation with At Least One Additional Risk Factor for Stroke • Age ≥ 75 years • Prior stroke, TIA or SE • CHF or LVEF ≤ 40% • Diabetes mellitus • Hypertension Randomize Double blind (n = 15,000) ARISTOTLE Apixaban placebo twice daily + Warfarin (target INR 2-3) Apixaban 5 mg oral twice daily + Warfarin placebo Warfarin/warfarin placebo adjusted by INR/sham INR based on encrypted point-of-care testing device Primary outcome: stroke and systemic embolism Other outcomes: Death, MI, bleeding Stratified by warfarin-naïve status 448 events over anticipated 2 year median follow-up; >90% power to show non-inferiority (apixaban vs warfarin upper bound of 95% CI <1.38)
Risk Factors • CHF • Hypertension • Age 75 • Diabetes OR • Stroke, TIA or Systemic embolus At least 2 required Atrial Fibrillation Rivaroxaban Randomize Double blind / Double Dummy (n ~ 14,000) Warfarin 20 mg daily 15 mg for Cr Cl 30-49 INR target - 2.5 (2.0-3.0 inclusive) Monthly Monitoring and adherence to standard of care guidelines Primary Endpoint: Stroke or non-CNS Systemic Embolism Statistics: non-inferiority, >95% power, 2.3% warfarin event rate