Download
1 / 4
40 likes | 53 Vues
In clinical utilizations of CAR T-cell treatment, perilous unfavorable occasions including cytokine discharge condition and neurotoxicity can prompt treatment disappointment. Results of patients treated with hostile to CD30 CAR T-cell have been baffling in backsliding/hard-headed (r/r) traditional Hodgkin's Lymphoma (cHL).

E N D
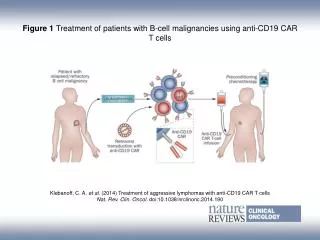
CD19 and CD30 CAR T-Cell Immunotherapy for High-Risk Classical Hodgkin's Lymphoma In clinical utilizations of CAR T-cell treatment, perilous unfavorable occasions including cytokine discharge condition and neurotoxicity can prompt treatment disappointment. Results of patients treated with hostile to CD30 CAR T-cell have been baffling in backsliding/hard-headed (r/r) traditional Hodgkin's Lymphoma (cHL). To comprehend the relevant populace of various CAR T-cell treatment, we analyzed the declaration of CD19, CD20, and CD30 CAR idiotype by immunohistochemistry (IHC) in 38 paraffin-implanted examples of cHL. In the previous two years, we discovered just a single patient with cHL who is
qualified for joined enemy of CD19 and CD30 CAR T- cell treatment. This present patient's standard attributes were inclined to serious unfriendly occasions. We treated this patient with low dosages and numerous mixtures of against CD19 and CD30 CAR T-cell. Results The positive articulation of CD19+ + CD30+ CAR idiotype in Reed-Sternberg (RS) cells is roughly 5.2% (2/38). The patient we treated with consolidated enemy of CD19 and CD30 CAR T-cell didn't encounter serious unfavorable occasions identified with CAR T-cell treatment and got long haul movement free endurance (PFS). For high danger r/r cHL patients, low dosages of CAR bb2121T-cell utilized over various days at various occasions may be protected and powerful. More clinical preliminaries are justified for CD19 and CD30 CAR T- cell blend treatment. Old style Hodgkin's Lymphoma (cHL) can be relieved utilizing standard chemotherapy with or without
radiation (1). Notwithstanding multi-modular treatment, 15–20% of patients with cHL surrender to this infection (2). The visualization for patients with cHL that are backsliding/recalcitrant (r/r) after first-line treatment or autologous undifferentiated cell transplantation (ASCT) is poor (3). Around 10–40% of patients don't accomplish a reaction to rescue chemotherapy and no randomized clinical preliminary information support ASCT in non-responders (4). Hence, it is basic to foster novel ways to deal with improve the anticipation for patients with r/r cHL. Hodgkin's lymphoma cells (mononucleated monster cell) or Reed-Sternberg (RS) cells are a run of the mill morphological element of cHL (5). The declaration of CD30 particles in RS cells is more noteworthy than 98% (1). Other than CD30, some B cells antigens, like CD19 and CD20, have been recognized in cHL (6). In spite of the fact that CD30 is humble communicated in ordinary tissues, it is specifically overexpressed in RS
cells, delivering this antigen a promising objective for novel treatment technique (3). Illusory antigen receptor (CAR) T-cell treatment is a successful technique for treating certain malignancies (7). Vehicles are ordinarily intended to perceive those antigens that are profoundly communicated in threatening cells (7–9). Vehicle consolidates an extracellular antigen-restricting space of a counter acting agent (scFv) with a transmembrane area, connected to at least one intracellular T-cell flagging areas (3). Sadly, clinical preliminary results in r/r cHL patients treated with hostile to CD30 CAR T-cell have been disillusioning (2, 3). As though yet, there is no clinical preliminary with CAR T-cell blend treatment for cHL.