Download
1 / 13
130 likes | 144 Vues
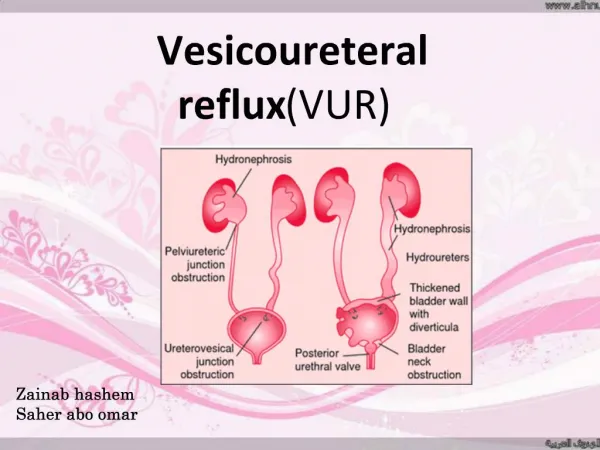
Kidney are important for urine formation. Normally, urine flows into the bladder through ureters. However, in some children, urine from the bladder flows back through the ureters. This condition is known as Vesicouretral reflux (VUR). It can be unilateral or bilateral.<br><br>http://www.pedsurgerydelhi.com/

E N D
Deflux In Reflux Dr Prashant jain
Vesicoureteric Reflux • Refers to a condition in which urine flows from the bladder BACKWARDS up the ureter and back into the kidneys • Primary: Due to defect in the uretero- vesical valves • Secondary: Neurogenic/Obstruction
Epidemiology of VUR the most common urologic finding in children, occurring in approximately 1% of newborns With UTI: About 30-45% of children have VUR following first confirmed UTI1 The reflux rate is 54% among girls ages 1 to 3 years with a history of febrile UTI2 The risk of febrile UTI recurrence is approximately 30% in children with grade III or IV reflux3-5 Recurrence rate may be lower in reflux grade I and II 5-10% of Pediatric ESRD is due to Reflux Nephropathy 1. Conway PH, et al. JAMA. 2007;298(2):179-186. 2. Jodal U. Infect Dis Clin North Am. 1987;1:713-729. 3. Pennesi M, et al. Pediatrics. 2008;121:e1489-1494. 4. Montini G, et al. Pediatrics. 2008;122:1064-1071. 5. Brandstrom P, et al. J Urol. 2010;184:286-291. 4
Symptoms Antenatal hydronephrosis Febrile UTI is a defining symptom Unexplained fever Urine dribbling between urinating Dysuria (pain on urination) Strong-smelling, cloudy, or bloody urine (hematuria) Abdominal, back, or side pain
VUR grades The severity of VUR is based upon a grading system, reflecting the extent of reflux and ureter abnormality1 • Kidney Kidney Kidney Kidney Kidney Ureter Ureter Ureter Ureter Ureter Bladder Bladder Bladder Bladder Bladder Grade I Grade II Grade III Grade IV Grade V More severe VUR is associated with more severe renal scarring and increased complications2,3 • 1AUA Guidelines 1997; 2Gonzalez 2005; 3Caione 2004
Renal Scarring • VUR + Pyelonephritis: The odds of renal scarring in children with VUR and pyelonephritis are 2.8 times greater than the odds of scarring for children with pyelonephritis without VUR. 7
Renal Scarring Increases with Severity of VUR Frequency (%) of Renal Scarring in Children Following Febrile UTI With Acute Lesions 78% 60% 47% Patients (N=161) included boys (n=41; mean age 1.2 years) and girls (n=120; mean age 2.9 years) with VUR grades 0 to V; no children had grade V reflux. Gonzalez E, et al. J Urol. 2005;173:571-574 8
Definition of success in VUR treatment Aim of treatment • Protect against febrile UTIs • Prevent renal scarring Definition of success • The successful prevention of febrile UTIs that could lead to renal scarring
VUR Treatment Options Prophylactic Antibiotics Open Surgery Endoscopic Injection Not Curative 5 – 13% Annual Resolution Curative 83% Success Rate** Curative 95% Success Rate Duration of Treatment 1 day (outpatient)1 Duration of Treatment 1 – 5 years* Duration of Treatment up to 3 days (inpatient)1 * Optimal duration of antibiotic prophylaxis is undetermined but clinical studies have used 1-5 years ** Majority of patients are cured after a single treatment 1Kobelt 2003
What is Deflux? • Viscous substance • Combination of Hyaluronic acid and Dextronomer • Bulking agent and coapts the ureteric orifice during bladder filling and emptying • Safe and well tolerated • Reproducible • No major adverse reactions • Does not alter the open surgery success 11
STING technique Submucosal plane of the INTRAVESICAL URETER 12
STING technique (Subureteric transurethral injection) The tip of the DEFLUX needle is inserted under the bladder mucosa 2 to 3 mm below the ureteral orifice at 6 o’clock position The needle tip is positioned in submucosal plane INTRAVESICAL URETER DEFLUX is prominent bulge appears and the orifice has a crescent-like shape . of the injected until a 13