Download
1 / 1
20 likes | 3.24k Vues
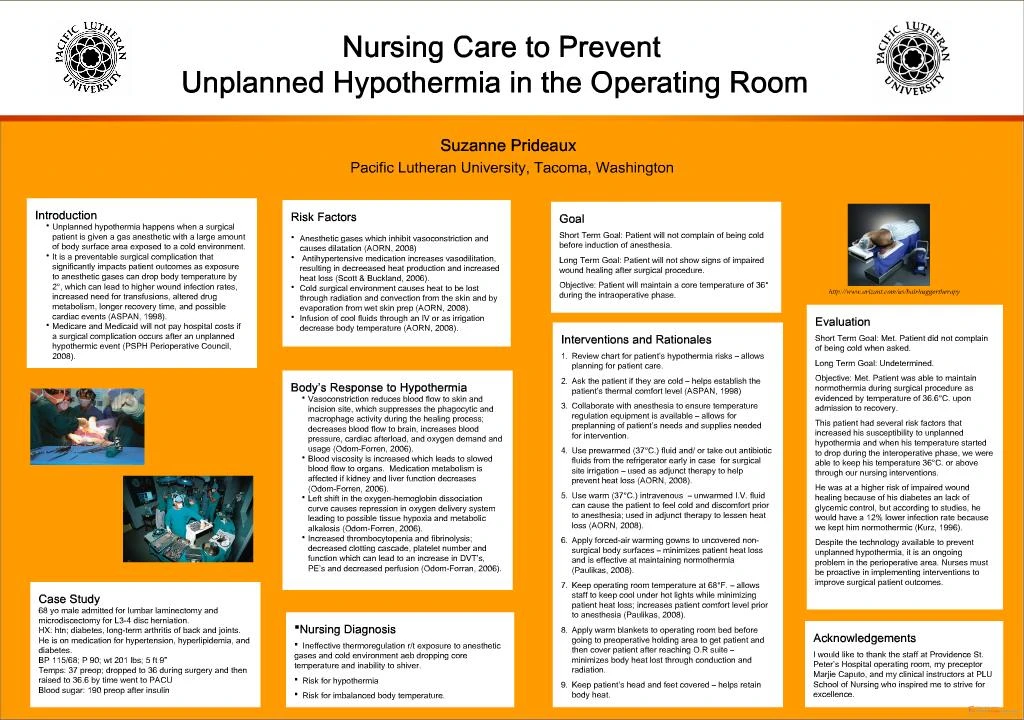
Cold surgical environment causes heat to be lost through radiation and ... case for surgical site irrigation used as adjunct therapy to help prevent heat ...

E N D