Back Pain
Back Pain. What is back pain ?. Any pain in the back. It is usually characterized by dull, continuous pain and tenderness in the lower lumbar, lumbosacral, or sacroiliac regions. Sometimes referred to the leg, following the distribution of the sciatic nerve. How Big Is the Problem?.


Back Pain
E N D
Presentation Transcript
What is back pain ? Any pain in the back. It is usually characterized by dull, continuous pain and tenderness in the lower lumbar, lumbosacral, or sacroiliac regions. Sometimes referred to the leg, following the distribution of the sciatic nerve.
How Big Is the Problem? • 2nd most common cause for GP visit . • 70% of the world adults will experience at least one disabling episode in their lives. • Each year, 15-20% will have back pain. • Most common cause of disability for persons < 45 years. • Disability due to back pain, particularly work absence, has increased significantly in the last 30 years.
How Big Is the Problem? • In western countries, back pain is the most common cause of sickness-related absences from work. • 8% of US population is disabled. • Costs to society: $20-50 billion/year. In UK: • 7% of adult population consult their GP each year with back pain. • Costs to society: £ 500 million/year. In US:
Classification of back pain Back Pain chronic recurrent acute
Acute V.S Chronic • Most acute episodes improve regardless of the treatment used, and the patient resumes normal activity within 6 weeks. • Chronic pain develops in only 10% to 15% of patients but it can cause significant distress and functional disability and requires aggressive treatment.
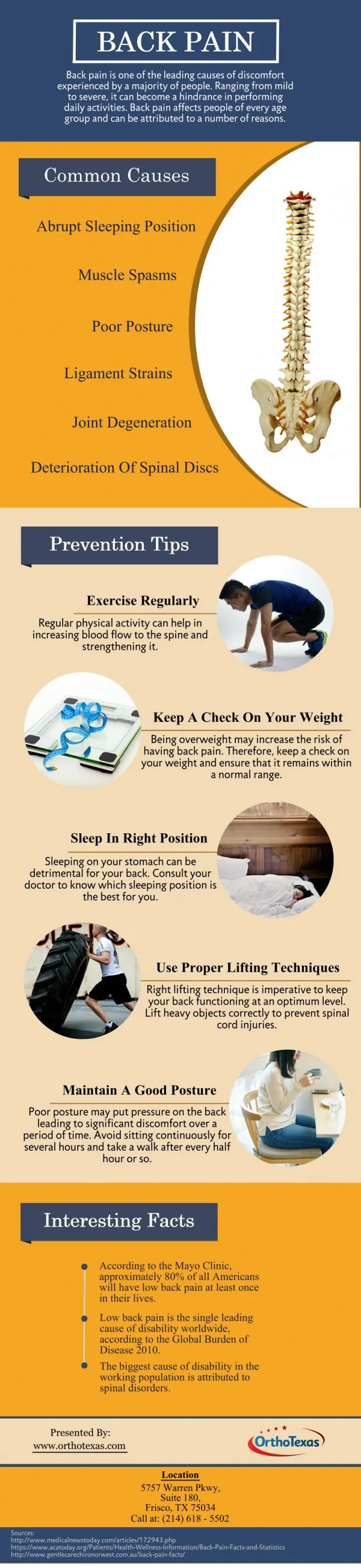
Causes of Back Pain Psychogenic factors (somatization) Systemic causes Back Pain uncomplicated Referred pain complicated
Uncomplicated Back Pain • Caused by some kind of structural problem (bone, muscle, joint, disc, nerves associated with lumber vertebrae or pelvis, tendon or ligament). • The most common mechanisms seem to be injury to muscles & ligament, osteoarthritis, degenerative disc disease, & malalignmet of spinal cord.
Injury to muscle & Ligaments • Includes strain, sprain or contusion of muscle and/or ligaments. • Occur when performing day-to-day activities, or from direct trauma such as a fall. • It the most common cause of acute low back pain, especially in young adults. • Patients with muscle & ligament injuries usually develop pain after unusual physical activity.
Degenerative Joint Disease (Osteoarthritis) • Is the most common cause of chronic low back pain in the elderly. • Loss of articular cartilage, osteophyte formation, and articular surface irregularity impair joint function and at times can lead to inflammation and pain. • Patients can experience pain in different situations (e.g. after unusual positioning or even while sleeping on a soft mattress).
Degenerative Disc Disease • Weakening of the fibrous outer ring of an intervertebral disc (the annulus fibrosus). • Can cause the gelatinous center of the disc ( the nucleus pulposus) to bulge or to herniate (extrude or rupture) into the spinal canal. • The discs most commonly involved are L3-L4, L4-L5, L5-S1.
Malaignment • Motion restriction of spinal structures such as the facet joints, the sacroiliac joint and/or the vertebral bodies.
Spondylolysis & Spondylolisthesis • Spondylolysis describes any sitution where there is a break in the integrity of the neural arch. • The principal cause is an aquired defect in pars interarticularis due to fracture. • Spondylolisthesis is where defect causes slippage of vertebra on the on below.
Other Causes • Fractures (usually a compression fracture of the vertebral body, often caused by minor trauma in older people with Osteoarthritis). • Type of occupations (workers in occupation requiring lifting heavy objects). • Smoking. • Obesity.
Complicated Back Pain • Structural with nerve root compromise (sciatica). • It is a condition in which pain, numbness, paresthesia &/or muscle weakness reflect injury to the spinal root or PN. • The most common cause is herniation of IV disc.
Spinal Stenosis • Back & leg symptoms associated with narrowing of the lumbar spinal canal seen on CT or MRI scanning. • The origin of the pain is may be related to bony pressure on multiple nerve roots, leading to ischemia of the nerves & pain. • The origin of the narrow canal may be congential.
Systemic Causes • Are rare (less than 1% of all cases). • They include cancer, infections, inflammatory arthritis and Paget’s disaese.
Referred Pain • Referred pain from abdominal or pelvic structures can arise from structures such as muscle, ligaments, or joint capsules. • The most common are: acute pancreatitis, pyelonephritis, pelvic inflammatory disease, dysmenorrhea, posterior peptic ulcer, abdominal aneurysm & cholecystitis. pain
Because the majority of physician visits for low back pain are to the GPs, family physician must has good skills in approaching, assessing & managing the patient with low back pain.
ربِ أوزعني أن أشكر نعمتك التي أنعمت علي وعلى والدي وأن أعمل صالحا ترضاه و أدخلني برحمتك في عبادك الصالحين .
Basic information about the patient • Name & address • Sex • Male: prostatic cancer, peptic ulcer disease,vertebral osteochondritis • Female:endometrosis,pregnancy,ovarian cancer • Age • young people :endometrosis,Ankolizing spodylitis • old people:multiple myleoma ,prostatic cancer
Occupation • Marital status.
Description of the presenting problem • Specify the main complain • Location • bilateral pain: sacroiliac joint disease. • psychogenic pain is not well localised. • Character • Radiation • To the lower limb :nerve root irritation . • Passing above flank region :kidney disease.
Duration of pain : • Most mechanical pain is intermittent • Medical conditions cause chronic pain that is persistent • Tumor of the spine : pain builds in intensity over months
History of the presenting complain • When did it start\onset of pain • Mechanical :acute sudden onset with mechanically disadvantaged position. • Medical causes: gradual slower onset. • Why do you thing you got it ? • Associated symptoms. • Numbness ,burning sensation :neural involvement.
Aggravating factor • Coughing ,sneezing,straining:nerve root irritation. • Bed rest: spondyloarthropathy –rolling over bed • Recumbency :tumor • Reliving factors. bed rest:herniating disc • Patients with psychogenic pain havedifficulty describing factors that relieve or worsen their pain.
Timing of the problem: • symptoms of joint compression is more sever by the end of day? • In the morning you are more in danger of getting disc herniation.? • inflammatory arthropathies :difficulty getting out of bed. • Patient with spinal tumors may get up during night and walk.
Review of body systems • Completely negative review is added evidence for mechanical nature of the pain. • Positive responses may indicate systemic cause • Weight loss • Cough /sputum • Abdominal pain • Bowel frequency • Rectal bleeding • Dysuria • Hematuria.
Fever with acute back pain (pyogenic sacroiliitis) • Menstural details • Weakness /numbness/wasting in the limbs
Previous medical history • Malignancy (breast –prostate) • Diabetes • Previous truma • Surgery(IV prolapse , urter stones ) • Previous investigation • Obstrectic history. • Contraception • History of steroid therapy.
Family history • Spondylarthropathies • Malignancy • Ethnic background • Caucasian women of Northern European are at greater risk of developing osteoporosis. • Omani?
Social history and occupational history • Workers doing heavy lifting are at risk of developing mechanical low back pain. • Drivers tend to develop musculoskeletal pain • Smoking and alcohol are associated with osteoporosis. • History of travel. • may infection. • may muscle stiffness
RED Flags • History of cancer • History of unexplained weight loss • History of fever, recent infection • History of immunosuppression • History of IV drug use • History of pain when supine; severe night pain • History of major trauma • History of minor trauma in elderly patient • History of recent bladder or bowel dysfunction • History of "saddle anesthesia" • History of severe or progressive neurologic motor andsensory deficits in legs
General Assessment • Starts the moment the patient enters the room till he sits . • Includes observation of the following; • Gait; watch the Pt walking (abnormal gaits) • Pt posture including the neck and trunk. (neck stiffness) • Assess erect position of head and smooth, coordinated neck movement. (Torticollis) • Way of sitting and facial expressions. (pain) • Proceed to system Examination. • Vital signs, skin. cvs, Rs, abdomen…,(WHY?)
Local Examination • Pt consentto fully expose . • Includes • Inspection • Palpation • Range of motion • Special maneuvers • Neurological examination. • Unexpected examinations ?!!!!!!!!!!!!!!!!!!!!
Inspection • Make sure • Pt is in upright position. • Feet together and arms hanging at the sides. • Head midline in the same plane as sacrum. • Shoulder and pelvis should be level. • Inspection of the spinal alignment • From the side. Findings • From behind. • Inspection of the skin. • Hairy patch? Pigmentation, dimpling vesicels?
Palpation • Think about the anatomical components. • Your aim is to palpate ; • The Bony prominence (the spine) • The muscles • Palpation of the spine is either by • Using the thumb Findings • Two fingers • Pal of the muscles is by using the two hands. • Findings. (painful areas, spasm or tightness).
Range of Motion • Assessed while the patient is still standing. • The neck than the spinal column. • Flexion (smoothness ,symmetry of movement, range of motion and curve in the lumber area)+ the degree. • Extension • Rotation. • Lateral bending.
Special Maneuvers • Leg Frezer test (hoover test). • Straight leg Raising test (mechanism and purpose ) • The crossed Straight leg Raising test.
Neurological examination • Involving the lower extremities specifically (why?) • Inspection • For each neurological level we shall test • The muscles power, reflexes and sensory areas.
Additional examination • The abdomen. • in males what else to be examined and why ? • In females and why? ¼ Bonus.
Remember It is never toooooo late for your lunch .
INVESTIGATIONS • DO YOU THINK THAT ALL PATIENTS WITH LOW BACK PAIN PRESENTING TO PRIMARY CARE PHYSICIAN NEED INVESTIGATIONS ? * MOST PATIENTS WITH LOW BACK PAIN DO NOT NEED INVESTIGATIONS.
INVESTIGATIONS • 1- Spinal X-rays * Are required only if the pain is associated with certain red flag symptoms or signs, which indicate a high risk of more serious underlying problems .
X- rays • If the pain : 1- Starts before the age of 20 or after 50 years. 2- Is persistent and a serious cause is suspected. 3- Is worse at night or in the morning , or when an inflammatory arthritis (e.g. ankylosing spodylitis) , infection or spinal tumour may be the cause. 4- Is associated with a systemic illness, fever or weight loss 5- Is associated with neurological symptoms or signs.
MRI & CT • Used when suspecting spinal cancer, herniated disc or infection. • MRI is preferable to CT scanning when neurological signs and symptoms are present. * Note : If red flags are present , MRI should be undertaken even if X-ray is normal.
INVESTIGATIONS • Bone scans • Useful in infection and malignancy • Full blood count, ESR and biochemical tests - Required only when the pain is likely to be due to malignancy , infection or a metabolic disease