Spinal Trauma A Pain in the Neck?
Spinal Trauma A Pain in the Neck?. James I. Syrett, MD, MBChB. George Lin, MD Office of Prehospital Care. Strong Memorial Hospital. Plan. Cases. Background. Spinal Injuries. Options for Immobilization. Clearing in the Field. Case. Patient A.

Spinal Trauma A Pain in the Neck?
E N D
Presentation Transcript
Spinal Trauma A Pain in the Neck? James I. Syrett, MD, MBChB. George Lin, MD Office of Prehospital Care. Strong Memorial Hospital.
Plan. • Cases. • Background. • Spinal Injuries. • Options for Immobilization. • Clearing in the Field.
Case • Patient A. • 57 year old male, drunk, restrained driver in a 60 mph impact into a tree. No airbag. • Mobile on scene. No pain. Aggressive to police.
Patient A • You are the first responder: What do you do?
Patient A • Airway • Breathing • Circulation • Total spine immobilization: C-collar, backboard • O2, IV, monitor
Patient A • Patient immobilized by EMS • Demand to be let off backboard. • Do you let him off?
Case • Patient A • Patient let off backboard due to no apparent injuries. • Patient sat upright. • Patient went into cardio-respiratory arrest. • Pronounced dead 27 minutes later.
Cases • Patient B. • Airplane crash with ejection of pilot. • Thrown from crash site. • Burns to hands. • Neck pain. • Chest pain.
Case • Patient B. • Backboard and collar. • Due to chest/lower back pain patient claimed could not breath, wants to be let off backboard and collar.
Patient B • What do you do? • Is it ok to let him off?
Case • Patient B. • Bilateral pneumothorax. • C5 fracture. • Multiple lumbar fractures.
Case • Patient C. • Transfer patient, fell 5 days ago. • Found to have C2 fracture at community hospital. • Transported by EMS without collar or backboard due to patient size.
Case • Patient C. • Found on arrival to have new paralysis from shoulder down. • Admitted to ICU. • Died from pneumonia 19 days later.
Why Talk About Spinal Trauma? • +200,000 spinal trauma victims living in the USA. • +10,000 new victims each year. • Annual cost to society is $5 billion each year. • The impact on victims and families is devastating.
Why? • “In the past, up to 10% of cases of permanent neurologic impairment after spinal trauma have been attributed to injudicious manipulation by paramedical personnel, examining physicians, or radiology technicians.” Robert S. Hockberger in Emergency Medicine, 4th Ed.
Where? • 50% Automobile/Motorcycle Accidents. • 20% Falls. • 15% Sports injury. • 15% Intentional Injury. • Median Age of Injury - 25 • Male:Female ratio - 4:1
Why? • First, DO NO HARM.
Why? • Second: Immobilization equipment is readily available to EMS, easy to use, relatively cheap and prevents further injury.
Why? • Third: It is the responsibility and the duty of EMS to ensure the patient gets to hospital in the same or a better condition than when they left the scene.
Hangman’s • Historically from Hangings • Extreme Hyperextension • Head On Collision and Sudden Deceleration • Unstable Fracture through Pedicle of C2: minimal cord injury
Wedge Fracture • Flexion • Anterior vertebral body injury/collapse • Stable fracture with minimal cord involvement
Teardrop Fracture • Flexion • Injury to anterior vertebral body: wedge shape fragment is displaced anteriorly • Unstable fracture: ligamentous injury
Clay Shoveler’s Fracture • Historically: Clay miners in Australia in 1930s when the lift heavy clay and flex their necks. • Flexion injury • Avulsion fracture of spinous process usually C7 • Stable
Spinal Emergencies • Diaphragmatic Paralysis • Bradycardia • Neurogenic Shock
Diaphragmatic Paralysis • C3 and above cord injury • C3,4,5 keep diaphragm alive • Secure airway • Provide respiratory support • Immobilization
Bradycardia • Sympathetic outflow cutoff • Atropine ready to patient side
Neurogenic Shock • Diagnosis of exclusion: rule out hemorrhagic shock, cardiac tamponade, tension pneumothorax • Usually mild • Trendelenburg’s position, IVF • Hospital setting: Dopamine/Levophed drip
When? • Mechanism of injury causing possible spinal trauma • MVC • Fall • Flash burn • GSW to neck • Stab wound to neck is usually not necessary • GSW to head usually not necessary • When in doubt, IMMOBILIZE
Aims of Immobilization. • Prevent further damage - Protect the Cord. • Hold the entire spine in a comfortable, anatomically correct and safe way. • Prevent movement of the entire spine. • Allow for safe concurrent management of other injuries.
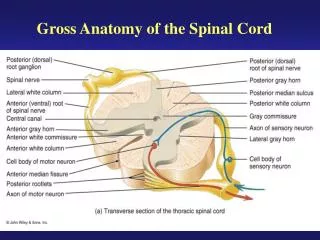
Options for Immobilization • Anatomical Regions (ENTIRE SPINE). • Head. • Neck. • Body.
Head. • Manual - Hands, Legs. • Simple Assist Devices - Sandbags, Towels, Foam Pads. • Additional Devices - Straps. • Head/Neck immobilizer.
Neck. • Collars. • Philadelphia. • Stiffneck. • Other options.
Body. • Backboards. • Hard, soft, shaped. • Short, long. • Kendrick Extrication Device. • Vacuum Splints.
Immobilization Principles. • No movement should be made that would worsen potential injuries. • No sudden movements. • No anatomically incorrect movements. • One at a time or careful coordination. • Make sure everyone knows what they are doing.
Immobilization Principles. • The patient should be transported in the position of maximum safety. • Children. • Football Players. • The Old Lady with Kyphosis.
Immobilization Principles. • The patient should be transported in a method that ensures the minimal amount of movement during transport. • Full Body Immobilization.
What is the Minimum Standard? • Airway with C-spine control. • Breathing. • Circulation. Advance Trauma Life Support 2000.
Clearing in the Field. • Benefits. • Reduction of on-scene time. • Reduction of ‘unnecessary’ transports. • Feeling of EMS autonomy.
Clearing in the Field. • Negatives. • Increased risk of litigation. • Cost of an error. • Difficulty in defining a standard that is known to work.
The NEXUS Study. • Patients required to meet 5 criteria. • No mid-line tenderness. • No focal neurological deficit. • Normal alertness. • No intoxication. • No painful, distracting injury.
NEXUS • Patients who underwent C-spine Xray for blunt trauma. • 34,069 patients included in study. • 818 patients had a C-spine injury. • 8 of these patients met all 5 criteria. • 4209 non-injured patients met all 5 criteria.
NEXUS • A good model for MDs with good insurance. • Bad model for EMS. • Scene stress. • Management stressors. • Failure to discriminate what pain is significant. • What is a distracting injury. • How drunk is intoxicated.