Download

1 / 63
670 likes | 2.03k Vues
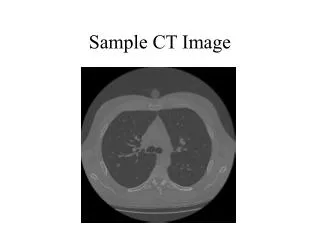
CT Image- guided injection techniques for spinal pain management. S. Bensoussan, MD, O. Silberman, MD. Department of Radiology, Bichat Hospital, Paris, France Tel Aviv Medical HOSPITAL Israel. Spinal pain and radiculopathy. Very common (prevalence = 5%/year) Most cases: Rest

E N D
CT Image-guided injection techniques for spinal pain management S. Bensoussan, MD, O. Silberman, MD Department of Radiology, Bichat Hospital, Paris, France Tel Aviv Medical HOSPITAL Israel
Spinal pain and radiculopathy • Very common (prevalence = 5%/year) • Most cases: • Rest • Physical therapy • Chiropractic manipulation • Percutaneous injection (under fluoroscopy control) Silbergleit et al, Radiographics 2001
Image CT guidance for percutaneous injections • Improves safety, success (1) • Indication: • Resistance to conventional therapy. • Resistance to steroid injection under fluoroscopy control at the lumbar spine • In first intention at the cervical and thoracic level • C indication to surgery • The last option before surgery ShulmanReg anesthes
Objective • To describe image guided techniques for spinal pain management under CT control)
Materials and Methods • 100 patients 20 – 58 y.o. diskherniation • Cervical and Lumbarlevel • Follow up AVS of 2 years 1 – 3 – 6 -12 and 24 months. • 70-80% of patients didn’tundergo to surgery. • 30% of this patients needed a second injection CT control • All the patients withendocanalar disc herniateweretreated in the sameprocedure by transligamentaryflavumpathway and foraminalpathway.
Materials and Methods • All Suffering from refractory persistent pain as diagnosed by above MD, despite of 1 month (at least) of appropriate medical treatment that included combination of analgesics, muscle relaxants and no inflammatory drugs, combined with physical therapy and for some of them, after steroid injection under fluoroscopy control.
Results: • Success: Radicular and lumbar or neck pain relief Serious complication= 0 (Phoneinterview 48h and 15 days after periradicular injection) AVS 0-10 • Within 2 weeks of periradicular injection most of patients returned to their previous occupation and full lifestyle
Results follow up after 2 years Full recovery : VAS between 0 and 2 Half recovery : VAS between 3 and 6 No recovery : VAS between 7 and 10
Indication • When there is a resistance towards conventional medical treatment while surgical intervention is to be recommended when neurological deficit becomes clear (LESS THAN 10% OF DISC HERNIATION) • Delmer.O,Dousset.V.,(2005),in Interventional Radiology in Pain Treatment, ch5:50-56,Kastler.B Ed, Spring Verlg berlin Heidelberg
Disc herniation, mecanism • The injury can result from a sudden strenuous movement, trauma, or after degenerative changes in the spine. • This kind of injuries is very common for professional athletes. • The result is a herniated disc that may compress, irritate or even permanently damage the nerve root. The severity and level of the lumbar disc herniation determines the type of signs and symptoms experienced by the patient. • Lumbar Disc herniations are seen in all age sport…..
Technic of the procedure • The skin entry site was marked with a surgical pen under sterile conditions, and 2% lidocaine was used for local anesthesia. • Three needles are introduced: • the 1st spinal needle is maneuvered directly adjacent to the involved nerve root in the outer neural foramen via a posterolateral approach, • The 2nd needle tip is introduced into the spinal canal by the trans yellow flavum ligamentary pathway.The needle tip is around the endocanal disc herniation.. • The 3rd foraminal needle is introduced at the superior or lower level of the disc herniation, considering the nerve root involved.
Transligamentaryflavum approach under ct control • TARGET: epidural space between ligament flavum, facet joint, disc herniation and symptomatic nerve root. • GOAL: to target accurately the inflammatory reaction around the nerve root and the disc herniation • PROCEDURE: Patients refered after a minimum of 1 month of adequate medical treatment, patient in a prone position axial scan to locate target slice.
Women 25 yo dancer Flavum ligamentum Left paracentral Disc herniation
Once optimal needles placements are achieved, a mixture of 7ml of methyl prednisolone with 0.5 mL of lidocaine 2% are introduced: 2ml via the 1st and the 3rd needles each, and 3 ml by the transligamentary pathway( 2nd needle). • A small contrast material (0.5ml) is being injected prior to bulk steroid injection (7ml) so that steroid diffusion would be assessed correctly. • The contrast injection was withheld if the patient is allergic. • The steroid drug is slowly injected so that it infiltrates efficiently the matrix around the nerve and the disc herniation. The needle is slowly withdrawn with pressure held by the radiologist. • The patients brought to the rest room for 30 min and his essential life parameters are monitored regularly. The patient is discharged to his home and advised to have rest for 3 days under a regime of noninflammtory drugs and paracetamol with gastric protectors .
Paramedian posterior approach and CT guided direct puncture from skin to the anterior aspect of the ligamentum flavum
Male 30 yoyoga instructorRight endocanalar L5-S1 disc herniation. Radiculopathy. No motor deficit • Needle tip in place • right flavum trans ligamentary pathway.
Cervical nerve root injection under Security CT control • Cervical radiculopathy is due to an abnormal process that involves the nerve roots • It is caused mostly by cervical disk herniation or uncarthrosis process in a lateral conflict. • The symptoms of cervical radiculopathy are neck and brachial-radicular pain, motor weackness or paresthesia , in 80-100 % of patients.
Cervical nerve root injection under Security CT control versus fluoroscopy • Foraminal cervical nerve root injection in patients who have persistent radicular pain without motor deficit, and should be performed only under CT guidance because of the presence of the vertebral artery. • CT guidance the once safety option (1) for cervical pain management because of the lack of visualization of the vessels and nerve root under fluoroscopy control (1)Complications of Cervical Selective Nerve Root Blocks Performed with Fluoroscopic Guidance Marc A. Wallace1, Melanie B. Fukui1, Robert L. Williams1, Andrew Ku1 and Parviz Baghai2 Department of Neurosurgery, Allegheny General Hospital, Pittsburgh, PA 2005
Cervical nerve root injection under Security CT control • The diagnosis of cervical radiculopathy was etablished by both the referring physicians and the interventional radiologist. • Radiographics, CT scan and MRI examinations performed to determine the causal lesions ,and exclude an anatomic variant, especially for vascular and bone structures. • Pregnant women and patients with cervical myelopathy,malignancy, inflammatories deasease, coagulation disturbances,or a history of severe corticosteroid side effects were excluded;
ForaminalSelective Nerve rootsteroid injection Vertebral artery (contrast) Male patient, 36 y.o. Left C6 radiculopathy C5-C6: small left postero-lateral disk herniation
MRI Axial ,Sag FSE T2 • W. 29 yo Right cervico brachial radiculopathy. No motor deficit. Axial MRI T2. C5-C6 Sagital MRI T2 Left postero-lateral disc herniation
Before needle injection THE FACET joint : The safe stopping point Because its situation is always posterior to the vertebral artery.
After needle injection Follow up 5 years No underwent to surgery One procedure was performed
Cyst injection Male patient, 50 years old Left L5 radiculopathy Left L5 nerve root compression by a left lumbar facet cyst MRI, FSE T2w L4-L5
Cyst injection Transarticular route
Cyst rupture 2 PROCEDURES WERE PERFORMED FOLLOW UP 4 YEARS : NO UNDERWENT TO SURGERY
Nerve root steroid injection Male patient, 35 y.o. golf player After bad movement Left back thoracic Pain. calcification T9-T10
Needle positioning Avoid pleural space ! (needle medial and posterior). Intra-discal and right nerve root calcifications
Control after 3 injections (one year after) Steroid injection
Fibrosis Post laminectomybilateral unremettingradiculopathy(spinal stenosis)
Discussion • Cervical and lumbar radiculopathy treated non surgically / ideal outcomes in 80-90% (1) • Surgery/ unremitting pain; progressive weackness or cervical myelopathy.(2) • cervical foraminal injections with antero-lateral approach under CT control • Ellenberg Arch Phys Med Rehab 1994
CT Guidance helps avoiding: • surgery in many cases (cervical thoracic and lumbar disc herniation, cyst facet joint)1,2,3 • complications usually due to lack of precision when using conventional fluoroscopy for guidance; • anaesthesia and sedation: most of the procedures are performed without any type of anaesthesia. 1-RSNA 2005 CT GUIDED TECHNICS for chronic cervico-brachialgia 2-AJNR Mars2004 Open study on Percutaneus Periradicular Foraminal steroid Infiltration under CT control in 30 patients 3-CARDIOVASCULAR AND INTERVENTIONAL radiology :CT-Guided Epidural/perineural Injections in Painful Disorders of the lumbar Spine
CT advantages • Accuracy • Safety (Preventing of harming delicate anatomic structures). • More accuracy under CT control between 30 to 40% than under fluoroscopy control.1 • The possibility to approach the endocanalar lesions by trans ligamentary pathway.
Conclusion • CT -guidance increases the precision of the procedure and help confirm needle placement. • Periradicular corticosteroid injections under CTimage-guided, complementarity step before more invasive treatment • an alternative to surgery.