Muscles part 1
E N D
Presentation Transcript
1 Muscles Muscles Part 1 Part 1 Prepare by Prepare by Dr. Mohammed Alruby Dr. Mohammed Alruby M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
2 Histology of muscles Physiology of muscles Muscles development Orofacial muscles -Facial muscles -Jaw muscles -Portal muscles Methods of studying muscles Muscle changes during growth Muscle function and facial development M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
3 Histology of muscles The structural and functional unit of the muscles is the muscle fiber Muscle fiber: elongated cylinder measure about 10 to 80 microns in thickness and from 1 to 15cm in length = Each muscle fiber contains an acidophilic granular cytoplasm (sarcoplasm) that rich in: Glycogen, mitochondria, Golgi apparatus, protein (actin, myosin, tropomyosin), Large number of myofibrils (sarcostyles) which responsible for muscle contraction = the muscle fiber is covered by thick membrane called (sarcolemma) and surrounded by CT called (endomysium) = the muscle fibers are coalescing together to form bundles; each bundles are covered by C T septa called perimysium = the muscle bundles are coalescing together to the whole muscle which is covered by CT fascia called epimysium, these CT contain: blood vessel, lymph vessel, and nerves, that firmly attach the muscle bundles to each other and attach the whole muscle to its tendon = the myofibrils (sarcostyles)are the contractile units of the muscle, in skeletal muscle they are transversely striated due to presence of dark and light bands The dark bands are formed of thick myosin filaments rich in Ca, the light bands are formed of thin actine filaments rich in water, there is a pale line in at the center of dark band called (Henesen’s disk), There is dark line at the center of light bands called (Krauses membrane) or Z line The distance between the two lines called (sarcomere) which is a contraction unit of the muscle. During the muscle contraction there the Sarcomere is shortened due to sliding of the light bands over the dark bans. The energy required for contraction is derived from transformation of ATP -- ---- ADP Physiology of muscles: Man has 639 muscles, composed of 6 billion muscle fibers, each fiber has 1000 fibrils, which means that there are 6000 billion fibrils at work at one of time or another. Elasticity: muscle can be stretched behind its original length and return to the original shape after relaxation (normal muscle can be elongated about 6/10 of its length Contractility: it is the ability of muscle to shorten its length under nerve impulse, this contraction is stimulated by acetyl choline, glycogen is partially oxidized to provides energy and lactic acid that carried away by blood stream Excessive accumulation of lactic acid can produce fatigue Isometric contraction: (stretching): the muscle is simply resisting the external forces without actual shortening Isotonic contraction: there is an actual shortening of the muscle, the strength of isometric contraction is much greater than that of isotonic contraction as the strength of contraction increase as the muscle being closer to the resting length Muscle tone: is the state of mild constant tension responsible for maintenance of various postures Stretch reflex: the reflex contraction of healthy muscle result from pull on its tendon All or non-law (Sherrington law): the individual muscle fibers have no variable contraction but they either relaxed or in maximum contraction, so that the strength of contraction depends on: -The number of muscle fibers involved in the contraction -Frequency of stimuli -The discharge from the individual muscle receptors (muscle spindle) M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
4 Neuromuscular reflexes: Reflexes is the basic unit of all neuromuscular activities, it is composed of receptors, afferent neuron, synaptic joint in the CNS, efferent neuron, effector organ Types of neuromuscular reflexes: 1-Conditioned reflexes: include all acquired reflexes that have been learned for example, thumb sucking 2-Unconditioned reflexes: include all reflexes that normally present at birth and are responsible for vital functions as: respiration, swallowing, sucking, sneezing, cough, gagging, tongue and mandibular postures. 3-Reflexes appearing with normal growth and development: as: Mature swallowing, mastication Muscle learning: The inherited muscle behavior is very difficult to be changed, but muscle can be learned anew conditioned reflexes through muscle training, the learning process involve three important steps: 1-The brain must have a clear image about the task to be performed (repeated training put the new reflexes into memory), this step involves conscious understanding of new skill 2-A new pathway must achieve for the new reflexes; this step involves reinforcement of new reflexes by repeated training 3-Central control of the new reflex must pass through the higher center of the brain (cerebral cortex), this step involves transition of the new skill to the unconscious level Muscles development: Prenatal development: The muscle grows by increase in size and amount of CT septa (endomysium, perimysium, epimysium) as well as cell division (increase in number of fibers) = Striated muscles begin to differentiate at 7th WIU, typical muscle fibers are seen at 22 WIU Normal muscle activity begins by the end of 7th MIU and still incomplete in extremities until after birth = The muscle increase by 59 folds from 4th MIU to birth and by 40 folds from birth to the middle of 3rd decade in postnatal life. This means that muscles achieve most of their growth in prenatal life. Post-natal development: Growth of muscles is rapid in infancy and early childhood, slower and regular in the middle and late childhood and again become more rapid before and during puberty. There is constant increase in the bulk of muscles from birth until maturity, this increase not equal in all muscles, the muscles of head show the smallest increments of the postnatal growth. From birth until 20 years old: -The facial muscles increase by 4 folds -Upper limbs by 16 folds -Lower limb by 24 folds N: B: In the middle of IUL, skeletal muscles represent 1/6 of total body weight At birth = 1/5 to ¼ of total body weight In early adolescent = 1/3 of total body weight At maturity: it equal 2/5 of total body weight M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
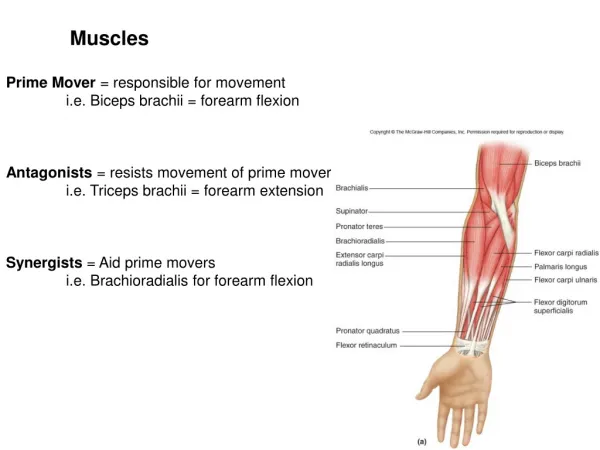
5 Orofacial muscles Origin: Some of the orofacial muscles are originated from the mesodermal myoblast of the first branchial arch Muscles of mastication developed in relation of the Meckel’s cartilage, attaching the forming mandible Genioglossus muscle arise from the membranous of the mandible and extended to tongue Geniohyoid muscle arise from the membranous of the mandible and extended to hyoid pre- cartilage Nerve supply: Facial muscles innervated by the 7th cranial nerve The jaw musculature innervated by the fifth cranial nerve Oral and pharyngeal muscle are innervated by fifth, ninth, tenth, cranial nerve Types: facial muscles, jaw muscles, portal muscles 1-Facial muscles: Introduction: The primary function of the facial muscles is expression of emotion; Coleman 1981 contends that human is capable of 7000 possible facial expression = It is important in maintenance of postures of facial structures, paralysis of the orbicularis oculi leads to dropping of the lower eyelids and drying of the conjunctiva Paralysis of the orbicularis oris muscles lead to angular chelosis = According to proffit 1987, the lips and the buccinator muscles opposed the tongue, contribute to postural equilibrium of the teeth = The facial muscles also contribute to stabilization of the mandible during infantile swallowing and in chewing and swallowing in the edentulous and occlusally compromised adult. = patient with short upper lip or excessively proclined upper incisors compensate by elevation of the lower lip through the action of the mentalis muscle to establish an anterior seal during swallowing = facial muscles also play an important role in both visual and spoken communication, the position of the chin and the inclination of the mandibular plane are controlled by the balance between the suprahyoid and the orofacial muscles. Since the posterior border of the ramus undergo gradual remodeling and maintains its normal inclination == N: B: Lider and Aronson reported that, the child with large adenoids may develop a mandible with a more open gonial angle, and later he observed that reduction of the angle occurs after adenoidectomy Types of orofacial muscles: 1-Orbicularis oris: Consists of numerous layers of muscle fibers surrounding the orifice of the mouth Origin: some of these fibers lie in other facial muscles and inserted into the lips. Other fibers developed from the mesenchymal tissues of the lips Action: compression of the lips producing distal force upon the incisors M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
6 2-Buccinator muscle: the muscle that coat the cheek Origin: Upper fibers: alveolar margin of maxilla above 3 molar teeth Lower fibers: alveolar margin of mandible below 3 molar teeth Middle fibers: the pterygo- mandibular ligament (raphe) N: B: pterygo mandibular ligament give attachment to the buccinator muscle anterior and to superior constrictor muscle of the pharynx posterior Insertion: Upper fiber: into the upper lip Lower fiber: into the lower lip Middle fibers: decussate at the angle of the mouth and pass to the upper and lower lip Actions: a-Draw the corner of the mouth laterally, pulling the lips against the teeth and flatten the cheek b-Exert inward force against the teeth to balance the very powerful force of the tongue c-Aids in swallowing by providing seal with the buccal teeth and prevent food from being entrapped in the mucobuccal sulcus during mastication d-Aids in whistling and blowing the trumpet e-Buccinator mechanism with superior constrictor and orbicularis oris muscle form a continuous band encircling the dentition and thus preventing them from carried for forward by the tongue and other occlusal forces N: B: --- there is a collection of fat on the bucco-pharyngeal fascia called buccal fate of pad on the outer surface of buccinator. It is larger on the suckling infant 3-Orbicularis oculi: formed of 3 parts: a-Orbital part: surrounding the orbital opening, act to close the eye tightly to avoid danger b-Palpebral part: lies in the eyelids, closing the eye gently c-Lacrimal part: surrounds the lacrimal sac, aspirate tears from conjunctival sac to the lacrimal sac 4-Quadratus labii superius: elevator superior alcanasi Origin: from the root of the nose Insertion: alar cartilage of the upper lip Action: raise the upper lip and the wings of the nose 5-Quadratus labii inferius: Origin: from the mandible below the canine and premolars Insertion: lower lip Action: pull the lower lip downward 6-Caninus: elevator anguli oris Origin: from canine fossa of the maxilla Insertion: orbicularis oris muscle Action: raise the corner of the mouth, draw it mesially 7-Zygomaticus minor: Origin: from the zygomatic bone just behind the zygomatico maxillary suture M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
7 Insertion: upper lip Action: raise the upper lip 8-Zygomaticus major: Origin: from zygomatic bone in front of zygomatico temporal suture Insertion: the angle of the mouth Action: pull the angle of the mouth upward and laterally as in smiling 9-Incisive labii superius: Origin: from maxilla above the canine and lateral incisor Insertion: into the orbicularis oris of upper canine 10-Incisive labii inferius: Origin: arise from the mandible below the canine and lateral incisor Insertion: into the orbicularis oris of lower lip Action: both superius and inferius are used to draw the corner of mouth mesially 11-Resorius muscle: Origin: from the subcutaneous tissue over the parotid gland Insertion: superficially at the corner of the mouth Action: pull the corner of the mandible laterally to produce the sardonic expression, it is a continuation of the platysma muscle in the face 12-Triangularis muscle: Origin: in the mandible below the canine, premolar, and first molar teeth Insertion: into the orbicularis oris Action: draw the corner of the mouth downward 13-Mentalis muscle: Origin: in the mandible below the lateral incisors Insertion: skin of the chin Action: draw the skin of the chin upward Wrinkle the skin of chin Draw the lower lip upward 2-Jaw muscles: Jaw muscles are often designated as elevator and depressor or protractor and retractor, EMG studies of postural position have shown that the infra mandibular group muscles are more active than the elevator muscle == the superior head pf lateral pterygoid muscles are illustrative of muscle’s multiple function. Calculation of this muscle vector about the instantaneous center of rotation suggest that its action early in opening and late in closure is to stabilize the joint == the functional protraction of the mandible in posture class II malocclusion that is called (Sunday bite) does not lead to skeletal correction == Moyers stated, {{what is the difference in adaptive stimulus between naturally occurring protrusive posture and that resulting from functional appliance? We do not know, but finding out would have a great clinical consequence, perhaps it is the frequent return of the mandible to more M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
8 dorsal position during mastication and swallowing which cancel the biologic signals to joint structures to adapt Types: 1-Masseter muscle: Origin: super-facial head: from the anterior 2/3 of the zygomatic arch Deep head: from the posterior and middle parts of the zygomatic arch Insertion: lateral surface of ramus of mandible Action: elevation and protraction of the mandible Superfacial fibers are used in incising The whole muscle in addition to the temporal muscles used in forceful contract at molars 2-Temporal muscle: Origin: from the temporal fossa of the temporal bone Insertion: into the medial surface of the coronoid process of the ramus Actions: a-Elevation and retrusion of the mandible. b-It is chiefly responsible for keeping the teeth in position and is constantly active when the person is in an upright position c-The anterior vertical fibers elevate the mandible upward, middle diagonal and posterior horizontal fibers elevate and retract the mandible to varying degree depending upon the direction of fibers involved in the contraction d-The posterior part of temporal muscle plays an important role in maintaining the mandibular postures and stabilization of the TMJ during rest as it closures to the joint e-Assist the lateral pterygoid muscle in the lateral movement by contralateral contraction on the other side. 3-The lateral pterygoid muscle: Origin: upper head: pterygoid plates of the greater wing of sphenoid bone and squama of infra temporal crest Lower head: lateral surface of lateral pterygoid plate of the sphenoid Insertion: upper head: the capsule of TMJ and the intra radicular disc Lower head: anterior aspect of condylar neck Actions: depress the mandible Pull the mandible forward and downward Unilateral contraction moves the mandible laterally Side to side movement by bilateral contraction 4-Medial pterygoid muscle: It has superfacial and deep heads embracing the lower head of lateral pterygoid muscle Origin: superfacial head: from maxillary tuberosity behind the last molar tooth Deep head: from the medial surface of lateral pterygoid plate Insertion: the two heads fuse and are inserted into the rough medial surface of the angle of the mandible Actions: bilateral contraction elevate the mandible Unilateral contraction moves the mandible from side to side Protrude the mandible M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
9 Adjustments of masticatory muscles: = the origins of masseter, internal pterygoid, and vertical fiber of the temporal muscle are separated by the mandibular condyle from their insertions = the origins of lateral pterygoid and horizontal fibers of the temporal muscles are separated by the growth of spheno-occipital synchondrosis = continuing growth of cartilage makes room for the developing muscles of mastication between the vertebral column and posterior portion of the facial skeleton = lateral growth of zygomatic arches also provides space for the muscles of mastication Summary of the masticatory actions: = the masseter, temporalis, and medial pterygoid muscles are elevator muscles used for closing the jaws, incising and grinding the foods = the infra mandibular muscles: regulate the position of mandible in space Acts against gravity Responsible for mandibular postures by their continuous unconscious tone = the posterior fibers of temporal muscle: stabilize the TMJ Regulate the position of the mandible during closure = retraction of mandible is achieved by contraction of posterior fibers of temporal muscle assisted by digastric and Geniohyoid muscles = protrusion of mandible is achieved by bilateral contraction of lateral pterygoid muscle assisted by anterior fibers of masseter = side to side movement is achieved by contraction of lateral or medial pterygoid muscle on one side and the contralateral contraction of temporal muscle on the other side = the mouth opening is achieved by contraction of lateral pterygoid muscle assisted by suprahyoid and digastric muscles N: B: Reciprocal innervation and inhibition phenomena exist between the elevator and the depressor muscles as: when the elevator muscles contract, there will be a controlled relaxation of the depressor muscle to allow smooth closing but not jerky 3-Portal muscles: The term portal area was coined by Bosma 1975 to denote the upper alimentary and respiratory tract, this muscles including the muscles of tongue, soft palate, pharyngeal pillar, pharynx proper and larynx The muscles of portal area are serve the multiple functions of postures, respiration and feeding Muscles of tongue: Origin: the tongue developed from the ventral mucous membrane of the 1st four branchial arches Development: anterior 2/3 formed by fusion of three process, two lingual process and one median process called tuberculum impar Posterior 1/3: mesenchymal condensation elevates from the second and third branchial arches to form copula (hypo branchial eminence). The copula and the endodermal mucosa of 2nd, 3rd and 4th branchial arches form the mucosa covering the posterior third of the tongue A-Extrinsic muscles: Origin: developed from occipital somite region and migrate to the area of developing tongue by myotomes migration M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
10 1-Hyoglossus muscle: Origin: from the hyoid bone Insertion: into the lateral side of the tongue Action: depress the tongue downward 2-Chondroglossus muscle: It is a small muscle which sometimes considered as a part of Hyoglossus muscle Origin: from the lesser cornu of hyoid bone Insertion: into the tongue Action: depress the tongue 3-Genioglossus muscle: Origin: from the superior genial tubercle of the mandible Insertion: into the medial part of the tongue along its whole length Action: protrude the tongue forward Depress the middle of the dorsal surface makes it as a concavity 4-Styloglossus muscle: Origin: from the styloid process and adjacent part of stylomandibular ligament Insertion: into the side of the tongue Action: raise the tongue upward and draw it back 5-Palatoglossus muscle: Origin: palatine aponeurosis Insertion: lateral side of the tongue Action: elevate the posterior part of the tongue N: B; Palatine aponeurosis: fibrous sheath attached to the posterior border of the hard palate, it thick and strong anterior but thin posterior B-Intrinsic muscles: 1-Superior longitudinal group: shorten the tongue 2-Inferior longitudinal group: shorten the tongue 3-Transverse longitudinal group: narrowing and elongate the tongue 4-Vertical longitudinal group: flatten and widen the tongue Muscles of pharynx: 1-Circular muscles: a-Superior constrictor muscle: Origin: medial pterygoid plate, pterygoid Hamulus, pterygo-mandibular raphe, lateral side of tongue Insertion: pharyngeal tubercle Action: constrict the pharynx b-Middle constrictor muscle: Origin: lesser and greater connu of hyoid bone Insertion: pharyngeal tubercle Action: constrict the pharynx c-Inferior constrictor muscle: M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
11 Origin: oblique line of thyroid cartilage and arch of cricoid cartilage Insertion: pharyngeal tubercle Action: constrict the pharynx 2-Longitudinal muscles: a-Salpingo-pharyngeous: Origin: cartilage of auditory tube Insertion: lateral wall of pharynx Action: elevate the pharynx in swallowing b-Palato-pharyngeous: Origin: posterior border of hard palate and palatal aponeurosis Insertion: lateral and posterior wall of the pharynx Action: elevate the pharynx in swallowing c-Stylo-pharyngeous: Origin: styloid process Insertion: upper and posterior surface of thyroid cartilage Action: elevate the pharynx in swallowing N: B: The bolus of food passes down through the pharynx by contraction of the superior and middle constrictor muscles in second stage of deglutition. In third stage, the inferior constrictor muscle contracts and relaxed to push the bolus down to the esophagus Muscles of palate: 1-Levator palati: Origin: petrous part of temporal bone, cartilaginous part of auditory tube Insertion: palatine aponeurosis Action: elevate the soft palate 2-Tensor palati: Origin: scaphoid fossa of the sphenoid bone, cartilaginous part of auditory tube Insertion: palatine aponeurosis Action: pull the soft palate to its side The muscles of two side acting together to stretch the soft palate, and depress it during the 1st stage of deglutition 3-Palatoglossus: Origin: palatal aponeurosis Insertion: lateral and posterior surface of tongue Action: depress the palate 4-Palato-pharyngeous: Origin: anterior part: arise from the posterior border of hard palate and under the surface of aponeurosis Posterior part: upper surface of aponeurosis Insertion: the two parts unite together and inserted to the posterior border of thyroid cartilage Action: elevate the pharynx in swallowing M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
12 5-Musculus uvulae: Origin: posterior nasal spine of palatine bone Insertion; mucosa of uvulae Action: elevate the uvulae Methods of studying muscles 1-Anatomic method: a-Gross section: The old method for studying the muscles, the shape, boundaries, origin and insertion provide insight into possible force vector of muscle, but estimated force vector for the whole muscle have limited value in predicting the real force vector, because the muscles are never fully contractile in normal function b-Histologic: Another traditional method of studying muscles, two major classifications are based on the concentration of oxidative enzymes and /or ATPase present in muscle fiber == on the basis of oxidative enzyme strains, fiber have been designated as: oxidative or glycolytic and functionally correlated with speed of contraction and susceptibility to fatigue Type I: Fiber are associated with small, low tension, slowly contracting motor unit These units are resistant to fatigue and richly supplied with capillary – this type depend on good circulation = fibers are found in significant proportion 30% only in the digastric muscle Type II: Fiber associated with large, high tension, rapidly contracting unit 1-Fatigue resistance and good capillary circulation: for maximum effort and long duration 2-Fatigue sensation and poor capillary circulation: for maximum effort and short duration = found in all jaws muscles and present in high proportions 45% in: -Superior posterior temporalis -Posterior medial pterygoid -Anterior digastric muscle 2-Functional method: a-Force and pressure: Pressures of the lips, cheeks and tongue against the teeth have been measured by number of investigators Masticatory, swallowing, and maximal biting forces have been recorded on teeth b-EMG: The most instrument used for evaluating the activity of oro-facial muscles, the electrical activity is easiest to record, electrode may be placed on the skin over the muscle or inserted into the body of the muscles 3-Behavioral: Mastication can be visualized as consolidation of simple elements such as jaw opening, jaw closing, jaw translation, tongue protraction, tongue retraction Other behavior such as swallowing appears to emerge as fully developed reflex to which other elements is added M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
13 In all animals: it appears that some behavior is predetermined and unlearned nest building of birds is predetermined while singing is learned from birds of the same species If sustaining behavior such as ventilation and swallowing are usually considered predetermined The bolus propelling component of swallowing appear to be predetermined while anterior seal and stabilization component are learned Muscles changes during growth Friel 1926, has shown correlation between the growth of muscles of mastication and the development of dentition, the muscles develop most rapidly after puberty when the deciduous teeth are replaced by the permanent dentition Skull deformity can be produced by pressure, removal paralysis of muscles, deformity is the result of changes in direction of growth of the developing skull Atrophy of the masticatory muscles due to injury or old age is responsible for change in shape of the mandible Subtleny found that soft tissue of the nose continuous to grow in downward and forward direction from age 1 to 18 years Continuous adjustment of muscle attachment during growth: = According to the type of attachment during growth, the muscles are divided into two groups: 1-Periosteal attachment: The muscle is directly attached to the fibrous layer of the periosteum; the muscles shift its attachment directly during growth 2-Tendinous attachment: The muscle is attached to the bone through a tendon The muscles shift its tendon by alternative bone deposition and resorption, the bone resorption freed the tendon and the muscle become temporarily periosteal, so the muscle can shift its tendon during growth maintaining its normal position after growth is ceases the muscle tendon is attached again to the bone N: B: = The mandible is attached to the cranium by the: - muscles of mastication. -sphenomandibular -stylomandibular -capsular ligament = the suprahyoid muscles are attaches are attached to inferior and lingual surface of the mandible and to the hyoid bone, where bone resorption is found in relation to tendinous attachment of muscle, resorption frees the muscle from the bone = muscles can become temporarily periosteal in attachment and can shift relative to bone growth maintaining their normal position, this is particularly true of muscle attached at the growing ends of the mandible = when resorption ceases, the muscles may become reattached directly to the bone by tendinous fibers N: B: M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby
14 Growth at the anterior end of each half of the mandible, until the symphyseal sutures is obliterated in the later part of the 1st year. Gradually tends to separate the anterior belly of digastric and Geniohyoid muscles The tendinous insertion of the temporal muscle is gradually freed from the bone of anterior border of the ramus of the mandible which is resorbed to make room for permanent molar eruption and the development of the alveolar process around these teeth The attachments of the internal pterygoid shifts during growth of the mandible and expand as the ramus increase in size by bone deposition along its posterior border Muscle function and facial development Prenatal muscle function: = with the differentiation of the neuromuscular system in the fetus, certain fetal movement are initiated in the forming muscles = when bone formation begins the neuromuscular contraction are effective in skeletal development = muscle function begins in intrauterine life: -influences the structural arrangement of the bones -induce the development of osseous process on the external surface of the bones. These changes may be brought about by bone apposition or resorption and are determined by endochondral growth center Post-natal muscle function: = from the age of 6 to 10 years of age, muscle development proceeds at steady rate = from age 10 to 15 years, development is less rapid = muscles developed rapidly in association with replacement of the deciduous dentition by the permanent one = failure of orbicularis oris to keep the lip closed in absence of other manifest causes may be due to a state of imbalance of the facial muscles secondary to mal-relationship of the jaws Nearly all humans show activity of their muscles of mastication during sleep. Contraction of muscles of mastication range from few to over 250 contractions within 8 sleep hours = force of pressure exerted during sleep ranges from 10 to 20 kg N: B: Phasic activities such as mastication, swallowing and speech are less likely to cause structural adaptation unless the force are heavy and /or act over long periods of time Bruxism: is an example of phasic activity which can cause structural changes in: -mastication -teeth -periodontal ligament -alveolar bone M Mu us sc clle es part 1 s part 1 Dr. Mohammed Alruby Dr. Mohammed Alruby