Download
1 / 46
630 likes | 3.03k Vues
Pelvic Organ Prolapse. Obstetrics & Gynecology 2005;106:615-634 OBGY R2 LEE EUN SUK. Abstract . Pelvic organ prolapse , including anterior and posterior vaginal prolapse, uterine prolapse, & enterocele, is a common group of clinical conditions affecting millions of American women.

E N D
Pelvic Organ Prolapse Obstetrics & Gynecology2005;106:615-634 OBGY R2 LEE EUN SUK
Abstract • Pelvic organ prolapse, including anterior and posterior vaginalprolapse, uterine prolapse, & enterocele, is a common groupof clinical conditions affecting millions of American women. • Pathophysiology of prolapseis multifactorial and may operate under a "multiple-hit" processin which genetically susceptible women are exposed to life eventsthat ultimately result in the development of clinically importantprolapse. • Evaluation of women with prolapse requires a comprehensiveapproach, with attention to function in all pelvic compartmentsbased on a detailed patient history, physical examination, andlimited testing. • Treatment is warranted based on specificsymptoms, prolapse management choices fall into 2 broad categories:nonsurgical, which includes pelvic floor muscle training andpessary use; & surgical, which can be reconstructive (eg,sacral colpopexy) or obliterative (eg, colpocleisis).
Clinical Importance • Based on projections from the United States Census Bureau, the number of American women aged 65 years and over will double in the next 25 years, to more than 40 million women by 2030 • Demand for health care services related to pelvic floor disorders will increased at twice the rate of the population itself • Although the overall rate of prolapse surgery has dropped, this represents a substantial drop in the rate of surgery for women less than 50 years old & a moderate increase for women aged 50 years and greater
Clinical Importance • Fig 1
Pathophysiology • Table 1
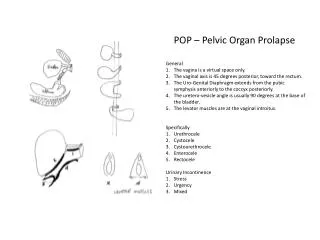
Diagnostic Approach • Women with prolapse often have urinary symptoms Some women have stress incontinence symptoms due to urethral incompetence, but many women, particularly those with advanced anterior vaginal prolapse, are continence • Defecatory symptoms such as excessive straining, incomplete rectal emptying, or the need for perineal or vaginal pressure to accomplish defecation • Influence of prolapse onsexual functioning should be addressed in women of all ages
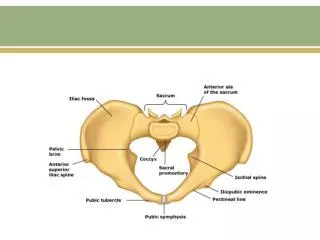
Diagnostic Approach • The extent of prolapse should be systematically assessed • With advanced prolapse, determining the extent of prolapse & its constituents ( anterior and posterior vagina; cervix or vaginal apex ) is usually not difficult • The use of vaginal speculums or retractors is very helpful in determining what vaginal sites are affected by prolapse • An unidentified vaginal bulge can be clearly identified as the vaginal apex, once the anterior and posterior vagina are retracted
Diagnostic Approach • fig2
Diagnostic Approach • fig3
Diagnostic Approach • fig4
Diagnostic Approach • The maximal extent of prolapse is demonstrated with a standing straining examination when the bladder is empty • Pelvic muscle function should be assessed after the bimanual examination → palpate the pelvic muscles a few centimeters inside the hymen, along pelvic sidewalls at the 4 & 8 o’clock Resting tone & voluntary contraction of the anal aphincters should be assessed during rectovaginal examination
Bladder Testing • At minimum, for all patients with prolapse, 3 pieces of information should be obtained; • Screening for urinary tract infection • Postvoid residual urine volume • Presence or absence of bladder sensation • Women with prolapse and urinary incontinence should have stress testing performed with the prolapse reduction because this will mimic bladder and urethral function when the prolapse is treated • In the setting of a positive reduction stress test → recommend that as incontinence procedure should be performed at the time of prolapse surgery
Indications for Treatment • Choice of treatment for prolapse depends on symptoms severity and severity of prolapse • Symptoms associated with stage I or II prolapse require careful evaluation, especially if surgery is being considered • Many women with stress urinary incontinence have stage I or II , although stress incontinence is not a symptom of prolapse ; it is simply a coincident symptom
Observation • Observation is appropriate for women whose symptoms are not sufficiently bothersome to warrant active management • There is no indications for treatment, particularly surgery, for women with asymptomatic prolapse “ before the problem gets any worse” • Occasionally a patient will present with advanced prolapse, yet she will say that she’s asymptomatic → is observation still qppropriate? • An important consideration is her efficiency of bladder emptying • Other risks : exposed vaginal epithelium & evisceration
Nonsurgical Management • Includes adjunct therapy to address concomitant symptoms, pelvic floor muscle training, and pessaries • Ideally, nonsurgical management will decrease the frequency and severity of symptoms, delay or avoid surgery & potentially prevent worsening the prolapse
Adjunct Therapy • Addresses symptoms of urinary, defecatory & sexual dysfunction • Patient often present with defecatory symptoms, such as excessive straining at stool and a feeling of incomplete evacuation, and physical examination reveals stage II or early stage III posterior vaginal prolapse (rectocele) → evaluation from the GI perspective • Age-appropriate screening for colorectal cancer : diet history (fiber and fluid intake), exercise history, review of medications for GI adverse effects, and bowel movements • Adjunct therapy includes advice on lifestyle alterations, weight loss, and a general exercise program
Pelvic Floor Muscle Training • Designed to increase the strength abd endurance of the pelvic muscles, thereby improving support to pelvic organs • “Kegel” exercises • With virtually no adverse effects, its only negative is the cost of providing instruction and follow-up for patients
Pessaries • To decrease symptom frequency and severity, delay or avoid surgery, and potentially prevent worsening of prolapse • The most important relative contraindication for pessary use occurs when the patient cannot comply with follow-up • Pessary use must be discontinued for persistent vaginal erosions • Unsuccessful fitting is associated with short vaginal length (less than 7cm) and wide introitus ( 4 finger-breadths)
Pessaries • Separated into 2 broad categories : support and space-filling • Ring pessary (with diaphragm) and other support pessaries are commonly recommended for stage II and early stage III • Space-filling pessaries such as the Gellhorn are usually used for more advanced prolapse • If some perineal support is preserved, a ring pessary ( without support when cervix is present, with support after hysterectomy) is good first choice
Pessaries • Gellhorn pessaries are useful for women with more advanced prolapse and less perineal support because they sometimes stay in place when ring pessaries do not • The Gellhorn is fitted so that the disk is centered in the upper vagina & the stem points downward behind the perineal body
Pessaries • The goal of changing the pessary at frequent intervals to prevent vaginal irritation that leads to discharge, infection, and erosion • If daily changing is too bothersome, a schedule of weekly or twice-weekly removal can be used • Vaginal estrogen is commly employed with pessaries • In women with vaginal atrophy at pessary initiation, local estrogen is important to prevent vaginal erosions
Surgical Management - Approach • Approach to prolapse surgery include vaginal, abdominal, and laparoscopic routes or combination of approaches • Vaginal approach results in fewer wound complications, less postoperative pain, shorter hospital stay, and less cost than abdominal surgery • Surgical procedures for prolapse : cathegorized into 3 groups • Restorative → use the patient’s endogenous support structures • Compensatory → replace deficient support with some type of graft • Obliterative → close the vagina
Prolapse Procedures –Anterior Vaginal Repair • Traditionally repaired with anterior colporrhaphy → vaginal epithelium separated from the underlying fibromuscular connective tissue, followed by midline plication of the vaginal muscularis with interrupted stitches → excision of excess epithelium & closure • Richardson reintroduced the concept of paravaginal repair → reattaches the anterior lateral vaginal sulcus to the obturator internus muscle and fascia at the level of the arcus tendineus fasia pelvis (“white line”) via transvaginal or retropubic access
Prolapse Procedures –Posterior Vaginal Repair • Traditionally posterior colporrhaphy → vaginal epithelium separated from the underlying fibromuscular connective tissue (rectovaginal septum, in between the vaginal muscularis and the rectovaginal adventitia) followed by midline plication of the vaginal muscularis with interrupted stitches → excision of excess epithelium & closure • Other procedures can be combined with posterior colporrhaphy, such as levator ani plication and peroneorrhaphy • Dyspareunia after posterior colporrhaphy → blamed on levator ani plication & narrowing can also occur with overzealous perineorrhaphy • The vaginal configuration is altered by the Burch procedure → the upward displacement of the anterior vaginal tube → create a transverse ridge in the posterior vagina
Burch Urethroplexy - Supporting the vagina (pubocervical fascia) beside the urethra is one of the two best cures for stress or activity related urine leakage
Prolapse Procedures–Posterior Vaginal Repair • Despite careful attention to ensure adequate introital caliber after posterior repair, 38% of women after Burch and posterior repair → persistent dyspareunia 1 year or more after surgery • Levator ani plication is associated with postoperative dyspareunia → recommend not to be performed in sexually active women • In non-sexually active women, levator ani plication performed to reinforce the repair, intentionally narrow the mid & lower vagina ; high perineorrhaphy can be added to further close the introitus
Prolapse Procedures–Vaginal Apical Repair • Apical vaginal prolapse includes uterine prolapse with or without enterocele and vaginal vault prolapse, typically with enterocele • The standard treatment for symptomatic uterine prolapse → hysterectomy with procedure to suspend the vaginal apex, address enterocele when indicated, repair coexisting anterior & posterior vaginal prolapse → perform anti-incontinence procedure
Enterocele Repair • Whether by vaginal, abdominal, of laparoscopic access, enterocele repair is traditionally performed by sharply dissecting the peritoneal sac from the rectum and bladder • A purse-string suture can be used to close the peritoneum as high as possible
Sacrospinous Ligament Suspension • Sacrospinous ligament fixation entails attachment of the vaginal apex to the sacrospinous ligament, the tendinous component of the coccygeus muscle
Iliococcygeal vaginal suspension • Iliococcygeal vaginal suspension involves attachment of vaginal apex to the iliococcygeus muscle and fascia, usually bilaterally
Uterosacral Ligament Suspension • Used prophylactically at hysterectomy or therapeutically for vaginal apical suspension • Once access to the posterior cul-de-sac has been attained, the uterosacral ligament remnant can be found • Sutures in each ligament and incorporated into the ant & post fibromuscular layer of vagina
Comparison of Vaginal Approaches to Apical Repair • Sacrospinous ligament suspension may leave the anterior vaginal at greater risk for subsequent failure & because the procedure is extraperitoneal → rare ureteral and rectal injury • Iliococcygeal suspension is straightforward procedure to learn and teach. It carriers virtually no risk of ureteral or small bowel injury, there are no vital structures nearby at risk for surgical injury • Uterosacral ligament suspension traditionally requires peritoneal entry → challenging in posthysterectomy prolapse, especially in the setting of bowel adhesions → engendering the rare occurrence of bowel injury • Uterosacral ligament suspension carreies a risk of ureteral injury (usually kinking due to medial displacement or suture ligation that impedes urinary flow)
Abdominal Apical Repair • Abdominal Sacral Colpopexy uses graft material attached to the anterior and posterior vaginal apex and suspended to the anterior longitudinal ligament of the sacrum for repair of apical prolapse • Peritoneal closure over the graft & obliteration of the cul-de-sac for treatment or prevention of enterocele • The cure rate range from 78% to 100% • Complications : intra-operative hemorrhage, laparotomy (adhesion & small bowel obstruction) , and graft infection or erosion
Comparison of Abdominal and Vaginal Approaches to Apical Repair • Success rates appear to favor the abdominal approach to apical vaginal prolapse • Abdominal sacral colpopexy is more durable in providing apical support, but at the cost of increased complications • Younger women benefit more also likely to be more from durability, with the reduced chance they will need prolapse surgery in future
Colpocleisis • In a healthy, sexually active woman the vagina may be surgically attached to the sacrospinous ligament, sacrum or fascia support system. But, they can be associated with occasional serious complications such as severe hemorrhage or major nerve injury • In those frail elderly women who do not wish to be sexually active in the future → total colpocleisis is a simple, safe, and effective surgical procedure that reliably relieves these women of their symptoms • Total colpocleisis procedure often coupled with a tension free vaginal tape (TVT) sling procedure for urinary incontinence
Diagnosis and Treatment of Stress Incontinence with Pelvic Organ Prolapse • Stress Incontinence (activity leakage) Loss of urine during coughing, sneezing, laughing or lifting something heavy. These activities cause an increase in "belly pressure“ → forces the urine out of the bladder Stress incontinence occurs almost exclusively in women & thought to be due to "pelvic (vaginal) relaxation" from childbirth or aging.
Diagnosis and Treatment of Stress Incontinence with Pelvic Organ Prolapse • Stress Incontinence - Treatments • Conservative TherapyPelvic Floor ExercisesUrinary Meatal Occlusion DevicesCollagen Injections • Urinary Incontinence SurgeryAnterior Repair and Kelly plicationPubovaginal Sling Procedures TVT Sling Surgical Procedures Burch Urethropexy Procedures • In an attempt to support the urethra, actually the vagina under and beside the urethra is the area which the operation takes place. The two most successful operations described → Pubovaginal Sling procedure & Burch urethropexy (colposuspension)
Adjunctive Materials • The most common prolase procedures using ajunctive materials are abdominal sacral colpopexy and anterior & posterior vaginal repairs • The ideal adjunctive material should be biocompatible yet inert, nonallergenic, noninflammatory, resistant to mechanical stress and conveniently available • It is critically important for surgeons to discuss the use of adjunctive materials with patients before surgery so patients are well-informed of risks and benefits and participate in the decision to use materials