Download
1 / 24
1.2k likes | 3.79k Vues
Kimberley Chien , MD Mercedes Martinez, MD Morgan Stanley Children’s Hospital of New York Reviewed by Melissa Jensen, MD of the Professional Education Committee. Biliary Atresia. Cases. 2 month old female referred by PMD presents with persistent jaundice

E N D
Kimberley Chien, MD Mercedes Martinez, MD Morgan Stanley Children’s Hospital of New York Reviewed by Melissa Jensen, MD of the Professional Education Committee Biliary Atresia
Cases 2 month old female referred by PMD presents with persistent jaundice • Ex-FT, no sig. maternal history, infection, c-section delivery complications • Feeding well: BM x 30 min every 2-3 hours • Mom feels stools were always light yellow, unchanged • Appropriate on growth curve • No meds • FH: +hiatal hernias, gastric ulcers • Of northern European descent; other siblings are healthy • No recent travel Achalasia Bisgard LD. Pediatrics in Review (2001)
Clinical Case Continued Physical exam: • Increased irritability but consolable • Mild-moderate jaundiced well nourished female with scleral icterus • II/VI systolic murmur at LSB appreciated; no radiation • +Hepatomegaly • Mildly acholic stool
Differential Diagnosis of Neonatal Cholestasis • Obstructive: • Biliary Atresia • Choledochal Cysts • Insippated bile/plug syndrome secondary to Cystic Fibrosis • Gallstone/biliary sludge • Tumors • Infections: • Toxoplasmosis • Rubella • CMV • Herpes • Syphilis • Echovirus • Adenovirus • Parvovirus B19 • Gram +/- bacteria • Genetic/Metabolic • Alagille Syndrome • Galactosemia • Tyrosinemia • Disorders of lipid metabolism • Disorders of bile acid metabolism • Mitochondrial disorders • Citrin deficiency • α-1 Antitrypsin deficiency • Neonatal hemochromatosis • Cystic Fibrosis • Parenteral Nutrition-associated Liver Disease • ARC syndrome
Definition Biliary Atresia A destructive inflammatory cholangiopathy where intrahepatic and extrahepatic bile ducts are destroyed at varying lengths during the neonatal period
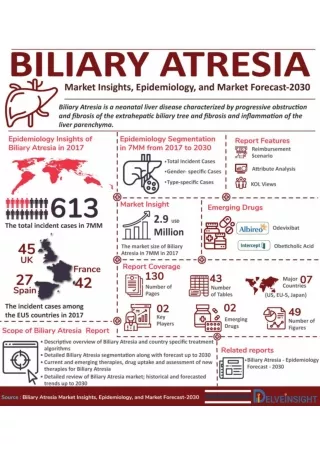
Epidemiology • Incidence: 1/10,000-20,000 live births in US • More common in East Asians • Screening measures desired for early detection and treatment • Tseng et al: Taiwanese study used stool color card screen • 46% decrease in very late referrals, decrease in Kasai operation occurring >90 days (9.5% vs. 4.9% after card implementation; P>0.05) • 90% of untreated patients die before 3 years of age • Average age of death: 19 months • Death due to cirrhosis and liver end-stage liver disease • 20% associated with other congenital malformations • 10% with Biliary Atresia Splenic Malformation (BASM) Syndrome
Possible Mechanisms of Pathogenesis • Viral: • Seasonal patterns that varied regionally suggest Rotavirus, Reovirus • CMV also suspected as possible culprit • Toxic: • Toxin-mediated inflammatory response causing BA in lambs of ewes who grazed on previously flooded areas • Genetic: • Increased frequency of CFC1 gene mutation involved in determining laterality during fetal development • Animal model of BA: transgenic mouse with deletion of inversin gene developed situs inversus and BA • Immunologic: • Increased maternal chimeric cells in portal/sinusoidal areas that may cause injury (i.e. graft-vs.-host response) • Polymorphisms that enhance CD14 gene expression • Up regulation of pro-inflammatory genes leading to significant inflammatory response in the liver and systemic circulation
Types of Biliary Atresia • Type I: • Common bile duct (CBD) is obliterated • Type IIa: • Atresia of common hepatic duct with patent cystic duct and CBD • Type IIb: • Atresia of common hepatic duct, cystic duct, and CBD • Type III: (>90%) • Patency to portahepatiswith discontinuity between right and left hepatic ducts
Clinical Manifestations Jaundice Acholic Stool Hepatosplenomegaly Growth Failure Dark Urine
Laboratory Findings • Conjugated hyperbilirubinemia > 2 mg/dl or >20% of total bilirubin level • Mild to moderate increases in serum aminotransferases • Disproportionately increased GGTP • Elevated Alkaline phosphatase • Initially, normal albumin and PT
Abdominal Ultrasound: to rule out other anatomic causes of cholestasis Findings consistent with biliary atresia Normal Gallbladder Irregularly shaped, shrunken gallbladder of 8 week infant with BA Triangular cord sign found in BA
Diagnostic Evaluation: Hepatobiliary Scintigraphy (HIDA Scan) HIDA scan of a patient with BA: Normal HIDA scan: Phenobarbital 5 mg/kg/day given for 3-5 days prior to optimize biliary excretion Positive finding: normal uptake in the liver and bladder, but failure to excrete tracer into the small bowel Not specific to BA
Diagnostic Evaluation: Liver Biopsy Bile duct proliferation and portal tract edema, inflammation and fibrosis Canalicular and bile duct plugs • Biopsy performed to determine Biliary Atresia from other possible causes of cholestasis • If biopsy is done too early in infancy, may have false negative results; may need to repeat at older age (e.g. 2 weeks later)
Diagnostic Evaluation: Intraoperative Cholangiogram • Gold standard • Determines patency proximally into the liver and distally into the bowel
Kasai: Hepatoportoenterostomy • Goal: To restore bile flow from the liver to the proximal small bowel
Kasai Hepatoportoenterostomy: First line of treatment • Initial studies show early treatment with Kasai improved outcomes and overall survival • Oh et al. • Infants with BA with Kasai <9 weeks after birth with better survival rates compared to those older at time of Kasai (83.3% vs. 35.3%; p<0.001) • Serinet et al. • Infants with BA and Kasai <45 days old had better outcomes • 12.1% difference in 15 year survival with native liver • Recent studies suggest delay in treatment does not significantly affect outcome • Despite controversy, recommend early diagnosis and treatment • Patients older than 90 days can still have 13% chance of survival with native liver
Poor Prognostic Factors Leading to Failure of Kasai • Late age at time of Kasai • Degree of fibrosis at time of Kasai • Development of cholangitis • Development of portal hypertension • Malnutrition • Portal pressure during Kasai • Presence of BASM • Anatomy of extrahepatic biliary remnant • Organization of post-op care • Access to liver transplant • Center experience
Potential Complications Post-Kasai • Ascending Cholangitis (Risk factor for poor outcome) • Direct contact between intrahepatic ducts and small intestinal tract and poor bile flow make more susceptible to cholangitis • Present with recurrence of jaundice, acholic stools, abdominal pain, signs of sepsis • Recurrent/late cholangitis suggest obstruction in Roux-en-Y • Hepatic fibrosis and cirrhosis • Present with signs of portal HTN (ascites, variceal bleeding) • Long term cirrhosis can lead to malignancy • Hepatopulmonary syndrome • Abnormal shunting in pulmonary vascular bed hypoxia and dyspnea
Post-Operative Care After Kasai • Success achieved if jaundice resolves by 3 months (good predictor of outcome) • Ursodeoxycholic acid (UDCA): • Improves bile flow • 15-30 mg/kg/day • Antibiotic prophylaxis: • 40-90% develop at least 1 episode of cholangitis • At risk due to abnormal anatomy, bacterial stasis • Trimethoprim/Sulfamethoxazole (4 mg/kg/day TMP;20 mg/kg/day SMX ÷2 times per day) • Neomycin (25 mg/kg/day ÷4 times per day) • If develop cholangitis, treat with antibiotics 4-6 weeks
Post-Operative Care After Kasai • Fat-Soluble Vitamin Replacement • Patients with persistent cholestasis are at risk for deficiency • Vitamin A, D, E, K supplements; monitor serum levels periodically • Can wean to standard vitamins when jaundice resolves and vitamin levels normalize after surgery • Nutrition Optimization • Contributing factors: malabsorption, chronic liver inflammation • Increased caloric needs of at least 150% recommended intake • Increased protein needs of 3-4 g/kg/day (infants) or 2-3 g/kg/day (children) • 40-60% of fat in meals should be MCT • Increasing caloric intake strategies: • Fortified breast milk, concentrated formulas (24-27 kcal/oz) • High-energy supplements or MCT oil • If po intake is not enough, may require NGT feedings • If NGT feedings not tolerated, strongly consider parenteral nutrition
Use of Steroids Post-Kasai • Steroids, used empirically, were thought to be standard of care in post-op period • Limited evidence: supported by numerous retrospective studies with varied methods • In 2007, randomized, double-blinded, placebo controlled study showed that corticosteroids had no significant effect on clearance of bilirubin or need for transplantation • In 2008, small prospective, open-labeled study with fixed dosing found corticosteroids to not be beneficial to post-Kasai survival of native liver, prevent the need for transplant, jaundice-free survival, true survival Davenport et al. Hepatology (2007) Petersen et al. Am J Gastroenterology (2008)
Liver Transplantation • Most common indication for pediatric liver transplantation • Indications for liver transplantation: • Primary failure of Kasai HPE • Persistent cholestasis at 3 months post-Kasai • Refractory growth failure • Worsening liver disease/Progressive biliary cirrhosis • Refractory ascites with respiratory dysfunction • Portal hypertension • Recurrent variceal bleeding • Recurrent cholangitis • Hepatopulmonary syndrome • Refractory coagulopathy
Liver Transplantation Outcomes • Patients with Biliary Atresia Splenic Malformation (BASM) do worse due to surgical complexity • Poor nutrition pre-op and post-op have increased mortality rates • In 2005, Barshes et al. reviewed 1,976 pts with BA in the US who received OLT • 1-, 5-, and 10-year survival was 90%, 87.2%, and 85.8% respectively • History of life support at time of OLT, and decreased age correlated with post-OLT mortality • This study did not find that living donor liver grafts were superior to cadaveric grafts (both split and partial/reduced) • Graft survival appeared to worsen in recent times vs. earlier times • This may be due to increase in the number of transplant centers; by decentralization, the center may be less equipped, less-skilled due to reduced surgeries performed per year
References • Barshes NR, Lee TC, Balkrishnan, Karpen SJ, Carter Baa, Goss JA. Orthotopicliver transplantation for biliary atresia: the US experience. Liver Transplantation(2005); 11(10): 1193-1200. • Baumann U, Ure B. Biliary atresia. Clinics and Research in Hepatology and Gastroenterology (2012); 36: 257-9. • Bisgard, LD. Visual diagnosis: a 10-week old infant who has jaundice. Pediatrics in Review(2001); 22: 408-12. • Caton AR, Druschel CM, McNutt LA. The Epidemiology of extrahepatic biliary atresia in New York State. 1983-98. Paediatric and Perinatal Epidemiology (2004); 18: 97-105. • Davenport M, Stringer MD, TizzardSA, McClean P, Miele-Vergani G, Hadzic N. Randomized, double-blind, placebo-controlled trial of corticosteroids after kasaiportoenterostomy for biliary atresia. Hepatology (2007); 46: 1821-7. • Harper P, Plant JW, Unger DB. Congenital biliary atresia and jaundice in lambs and calves. Aust Vet J .(1990); 67(1):18. • Hartley JL, Davenport M, Kelly DA. Biliary atresia. Lancet (2009); 374: 1704-13. • Meyers RL, Book LS, O’Gorman MA, Jackson WD, Black RE, Johnson DG, Matlak ME. High-dose steroids, ursodeoxycholic acid, and chronic intravenous antibiotics improve bile flow after kasai procedure in infants with biliary atresia. J PedSurg(2003); 38(3): 406-11. • Oh M, Hobeldin M, Chen T, Thomas DW, Atkinson JB. Kasai Procedure in the treatment of biliary atresia. J Pediatric Surgery (1995);30(7):1077-81. • Petersen C, Harder D, Melter M, Becker T, Wasielewski RV, Leonhardt J, Ure BM. Postoperative high-dose seteroids do not improve mid-term survival with native liver in biliary atresia. Am J Gastroenterology (2008); 103: 712-9. • Serinet MO, Wildhaber BE, Broue P, LachauxA, Sarles J, Jacquemin E, Gauthier F, Chardot C. Impact of age at Kasai operation on its results in late childhood and adolescence: A rational basis for biliary atresia screening. Pediatrics (2009); 123: 1280-6. • Shneider BL, Brown MB, Haber B, Whitington PF, Schwarz K, Squires R, Bezerra J, Shepherd R, Rosenthal P, Hoofnagle JH, Sokol RJ, Biliary Atresia Research Consortium. Multicenter study of the outcome of biliary atresia in the united states, 1997-2000. J Pediatrics (2006); 148(4): 467-474. • Sullivan JS, Sundaram SS, Pan Z, Sokol RJ. Parenteral nutrition supplementation in biliary atresia patients listed for liver transplantation. Liver Transplantation(2012);13: 121-9. • Tseng JJ, Lai MS, Lin MC, Fu YC. Stool color card screening for biliary atresia. Pediatrics(2011); 129: e1209-15.