Peripheral Neuropathy
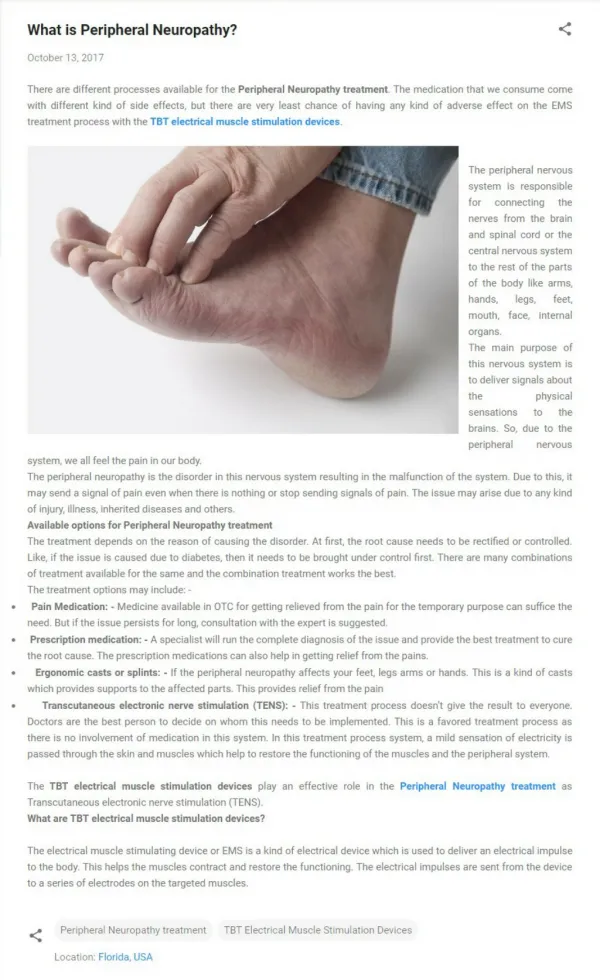
Peripheral Neuropathy. Victor F. Politi, M.D., Medical Director, St. Anthony’s School of Allied Health Professions, Physician Assistant Program. Introduction. Peripheral neuropathy describes damage to the peripheral nervous system.

Peripheral Neuropathy
E N D
Presentation Transcript
Peripheral Neuropathy Victor F. Politi, M.D., Medical Director, St. Anthony’s School of Allied Health Professions, Physician Assistant Program
Introduction • Peripheral neuropathy describes damage to the peripheral nervous system. • More than 100 types of peripheral neuropathy have been identified, each with its own characteristic set of symptoms, pattern of development, and prognosis.
Introduction • Impaired function and symptoms depend on the type of nerves • motor, sensory, or autonomic • that are damaged.
Introduction • Motor nerves • control movements of all muscles under conscious control, such as those used for walking, grasping things, or talking. • Sensory nerves • transmit information about sensory experiences, such as the feeling of a light touch or the pain resulting from a cut. • Autonomic nerves • regulate biological activities that people do not control consciously, such as breathing, digesting food, and heart and gland functions.
Introduction • Although some neuropathies may affect all three types of nerves, others primarily affect one or two types. • Therefore, terms such as • predominately motor neuropathy • predominately sensory neuropathy • sensory-motor neuropathy • autonomic neuropathy • are often used to describe a patient's condition.
Introduction • Because every peripheral nerve has a highly specialized function in a specific part of the body, a wide array of symptoms can occur when nerves are damaged. • Some people may experience temporary numbness, tingling, and pricking sensations (paresthesia), sensitivity to touch, or muscle weakness.
Introduction • Others may suffer more extreme symptoms, including burning pain (especially at night), muscle wasting, paralysis, or organ or gland dysfunction.
Introduction • People may become unable to digest food easily, maintain safe levels of blood pressure, sweat normally, or experience normal sexual function. • In the most extreme cases, breathing may become difficult or organ failure may occur.
Introduction • Some forms of neuropathy involve damage to only one nerve and are called mononeuropathies. • More often though, multiple nerves affecting all limbs are affected-called polyneuropathy.
Introduction • Occasionally, two or more isolated nerves in separate areas of the body are affected-called mononeuritis multiplex.
Introduction • In acute neuropathies, such as Guillain-Barré syndrome, symptoms appear suddenly, progress rapidly, and resolve slowly as damaged nerves heal. • In chronic forms, symptoms begin subtly and progress slowly.
Introduction • Some people may have periods of relief followed by relapse. • Others may reach a plateau stage where symptoms stay the same for many months or years.
Introduction • Some chronic neuropathies worsen over time, but very few forms prove fatal unless complicated by other diseases. • Occasionally the neuropathy is a symptom of another disorder.
Introduction • In the most common forms of polyneuropathy, the nerve fibers most distant from the brain and the spinal cord malfunction first. • Pain and other symptoms often appear symmetrically, for example, in both feet followed by a gradual progression up both legs.
Introduction • Next, the fingers, hands, and arms may become affected, and symptoms can progress into the central part of the body. • Many people with diabetic neuropathy experience this pattern of ascending nerve damage.
Anatomy • The body’s nervous system is made up of two parts. • The central nervous system (CNS) • The peripheral nervous system (PNS)
Anatomy • The peripheral nerves include: • cranial nerves • (with the exception of the second) • spinal nerve roots • dorsal root ganglia • peripheral nerve trunks and their terminal branches • peripheral autonomic nervous system
Diagnostic Approach • The differential diagnosis of peripheral neuropathy is significantly narrowed by a focused clinical assessment that addresses several key issues – • Does the patient actually have a neuropathy? • What is the pattern of involvement? • Is the neuropathy focal, multifocal or symmetric? • If the neuropathy is symmetric, is it proximal or distal?
Diagnostic Approach • Does the patient actually have a neuropathy? • Causes of generalized weakness include motor neuron disease, disorders of the neuromuscular junction and myopathy. • Peripheral neuropathy can also be mimicked by myelopathy, syringomyelia or dorsal column disorders, such as tabes dorsalis. • Hysterical symptoms can sometimes mimic a neuropathy.
Diagnostic Approach • Is the neuropathy focal, multifocal or symmetric? • Focal neuropathies include common compressive neuropathies such as carpal tunnel syndrome, ulnar neuropathy at the elbow or peroneal neuropathy at the fibular head • A multifocal neuropathy suggests a mononeuritis multiplex that may be caused, for example, by vasculitis or diabetes
Diagnostic Approach • If the neuropathy is symmetric, is it proximal or distal? • Most toxic and metabolic neuropathies present as a distal symmetric or dying-back process. • Proximal sensory neuropathies are rare and include porphyria. • Predominantly motor neuropathies are often proximal and include acquired inflammatory neuropathies such as Guillain-Barré syndrome. • An exception is lead neuropathy, which initially affects motor fibers in radial and peroneal distributions.
Infectious diseases Acquired immunodeficiency syndrome Lyme disease Sarcoidosis Toxic neuropathy Acrylamide Carbon disulfide Dichlorophenoxyacetic acid Ethylene oxide Hexacarbons Carbon monoxide Organophosphorus esters Glue sniffing Metal neuropathy Chronic arsenic intoxication Mercury Gold Thallium Medications (see next slide) Distal Symmetric Sensorimotor Polyneuropathies
AxonalVincristine (Oncovin, Vincosar PFS) Paclitaxel (Taxol) Nitrous oxide Colchicine (Probenecid, Col-Probenecid) Isoniazid (Laniazid) Hydralazine (Apresoline) Metronidazole (Flagyl) Pyridoxine (Nestrex, Beesix) Didanosine (Videx) Lithium Alfa interferon (Roferon-A, Intron A, Alferon N) Dapsone Axonal - continued..Phenytoin (Dilantin) Cimetidine (Tagamet) Disulfiram (Antabuse) Chloroquine (Aralen) Ethambutol (Myambutol) Amitriptyline (Elavil, Endep) DemyelinatingAmiodarone (Cordarone) Chloroquine Suramin (Fourneau 309, Bayer 205, Germanin) Gold NeuronopathyThalidomide (Synovir) Cisplatin (Platinol) Pyridoxine Medications Causing Neuropathies
Proximal Symmetric Motor Polyneuropathies • Guillain-Barré syndrome • Chronic inflammatory demyelinating polyradiculoneuropathy • Diabetes mellitus • Porphyria • Osteosclerotic myeloma • Waldenstrom's macroglobulinemia • Monoclonal gammopathy of undetermined significance • Acute arsenic polyneuropathy • Lymphoma • Diphtheria • HIV/AIDS • Lyme disease • Hypothyroidism • Vincristine (Oncovin, Vincosar PFS) toxicity
Diagnostic Approach • Neuropathies can be categorized according to the fiber type that is primarily involved. • Most toxic and metabolic neuropathies are initially sensory and later may involve the motor fibers.
Diagnostic Approach • Pure sensory neuropathies can result from drug toxicity (e.g., thalidomide, cisplatin [Platinol]), paraneoplastic syndromes or nutritional deficiencies. • Primarily motor neuropathies include Guillain-Barré syndrome.
Diagnostic Approach • Alcoholism and diabetes can both cause small-fiber, painful neuropathies
Diagnostic Approach • Autonomic involvement occurs in many small-fiber neuropathies but can also occur in Guillain-Barré syndrome and is sometimes life-threatening.
Diagnostic Approach • It is important to distinguish whether the neuropathy is axonal, demyelinating, or both. • This differentiation is best achieved using nerve conduction studies (NCS) and electromyography (EMG).
Diagnostic Approach • Diabetes, HIV infection and alcoholism can cause several patterns of neuropathy. • They most commonly cause a distal, symmetric axonal sensorimotor neuropathy. • The second most common presentation in these conditions is a small-fiber, painful neuropathy.
History • The temporal course of a neuropathy varies, based on the etiology. • With trauma or ischemic infarction, the onset will be acute, with the most severe symptoms at onset. • Inflammatory and some metabolic neuropathies have a subacute course extending over days to weeks. • A chronic course over weeks to months is the hallmark of most toxic and metabolic neuropathies.
History • A chronic, slowly progressive neuropathy over many years occurs with most hereditary neuropathies or with chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). • Neuropathies with a relapsing and remitting course include Guillain-Barré syndrome.
History • Ischemic neuropathies often have pain as a prominent feature. • Small-fiber neuropathies often present with burning pain, lightning-like or lancinating pain, aching, or uncomfortable paresthesias (dysesthesias).
History • Dying-back (distal symmetric axonal) neuropathies initially involve the tips of the toes and progress proximally in a stocking-glove distribution.
History • Peripheral neuropathy can present as restless leg syndrome. • Proximal involvement may result in difficulty climbing stairs, getting out of a chair, lifting and swallowing, and in dysarthria.
History • The clinical assessment should include: • careful past medical history, looking for systemic diseases that can be associated with neuropathy, such as diabetes or hypothyroidism.
History • Many medications can cause a peripheral neuropathy, typically a distal symmetric axonal sensorimotor neuropathy. • Detailed inquiries about drug and alcohol use, as well as exposure to heavy metals and solvents, should be pursued.
History • All patients should be questioned regarding • HIV risk factors • foreign travel (leprosy) • diet (nutrition) • vitamin use (especially B6) • possibility of a tick bite (Lyme disease)
History • The review of systems may provide clues regarding other organ involvement and the presence of an underlying malignancy.
Physical Examination • A cranial nerve examination can provide evidence of mononeuropathies or proximal involvement. • Funduscopic examination may show abnormalities such as optic pallor, which can be present in leukodystrophies and vitamin B12 deficiency.
Physical Examination • Direct strength testing of muscles enervated by cranial nerves V, VII, IX/X, XI and XII is important, as mild bilateral weakness can be missed by observation only.
Physical Examination • The motor examination includes a search for fasciculations or cramps, or loss of muscle bulk. • Tone is normal or reduced.
Physical Examination • The pattern of weakness helps narrow the diagnosis: symmetric or asymmetric, distal or proximal, and confined to a particular nerve, plexus or root level.
Physical Examination • Deep tendon reflexes are reduced or absent. • A bilateral foot drop may result in a steppage gait in which the patient must lift the knees very high in order to clear the toes. • Proximal weakness results in an inability to squat or to rise unassisted from a chair.
Physical Examination • The general physical examination can provide evidence of orthostatic hypotension without a compensatory rise in heart rate when autonomic fibers are involved.
Physical Examination • Respiratory rate and vital capacity should be evaluated in Guillain-Barré syndrome to assess for respiratory compromise. • The presence of lymphadenopathy, hepatomegaly or splenomegaly, and skin lesions may provide evidence of systemic disease.
Physical Examination • Pale transverse bands in the nail beds, parallel to the lunula (Mees' lines), suggest arsenic poisoning.
Laboratory Evaluation • EMG and nerve conduction studies (NCS) are often the most useful initial laboratory studies in the evaluation of a patient with peripheral neuropathy
Laboratory Evaluation • They can confirm the presence of a neuropathy and provide information as to the type of fibers involved (motor, sensory, or both), the pathophysiology (axonal loss versus demyelination) and a symmetric versus asymmetric or multifocal pattern of involvement.