Evaluating for Developmental Delay
Evaluating for Developmental Delay. Jimmy Treadway MD. Introduction. An estimated 12-16% of children have a developmental and/or behavior disorder Only 30% are identified before school entrance

Evaluating for Developmental Delay
E N D
Presentation Transcript
Evaluating for Developmental Delay Jimmy Treadway MD
Introduction • An estimated 12-16% of children have a developmental and/or behavior disorder • Only 30% are identified before school entrance • Those detected after school entrance miss out on early intervention services proven to have long term health benefits • Pediatricians are the primary professional with whom families have contact during a child’s first five years of life • Early identification by primary care providers of developmental delays leads to early referral for evaluation and treatment
Introduction • The Individuals With Disabilities Education Act (IDEA) Amendments of 1997 mandates early identification and intervention for developmental disabilities and requires clinicians to refer children with suspected developmental delays to the appropriate early intervention system in a timely manner • An established diagnosis of development disability is not necessary for referral to early intervention programs
Introduction • Developmental Disability/Delay (DD)is present when functional aspects of a child’s development in one or more domains (gross/fine motor, speech/language, cognition, social/personal, and activities of daily living) are significantly delayed compared to the expected level for age (≥25% from the expected rate or a discrepancy of 1.5 to 2 standard deviations from the norm)
Introduction • Global Developmental Delay (GDD) is a subset of DD defined as significant delay in two or more developmental domains (reserved for children less than 5 years old)
Surveillance and Screening • In any patient population, there are children with normal development, children with obvious abnormal development and those in between • Pediatricians are in unique position to provide surveillance and screening due to their routine contact with children and their families • The American Academy of Pediatrics (AAP) recommends all infants and young children have surveillance/screening for developmental delays
Surveillance and Screening • Surveillance—the identification of risk factors for DD • Should be performed at all well child visits Includes: • Attending to parental concerns • Obtaining relevant developmental history • Making accurate observations of the child • Sharing concerns with other professionals • Maintaining record of findings • Provides the context for screening tests
Surveillance and Screening • Evidence based surveillance • Psychosocial risks can be evaluated with measures such as the Family Psychosocial Screen (FPS) • ~15 minutes • ≥4 risk factors are associated with DD • Parental Concerns can be evaluated with measures such as the Parents’ Evaluation of Developmental Status (PEDS) • 10 questions, ~2minutes • Scores indicate if a child is at high, moderate, or low risk for DD
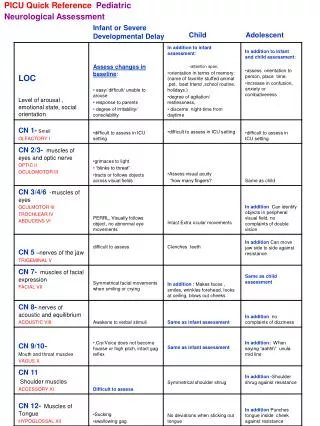
Surveillance and Screening • Medical Evaluation • Presence of biologic risks or medical problems associated with DD • Head circumference for micro/macrocephaly • Weight and height for growth deficiency • Dysmorphology (minor and major congenital abnormalities) • Eye exam for poor tracking, strabismus, etc • Ear exam for recurrent/chronic OM • Abdomen for HSM (metabolic disease) • Skin for neurocutaneous lesions • Neurologic exam for reflexes, tone, symmetry, strength
Surveillance and Screening • Screening—brief, formal, standardized evaluation for early identification of deviations from normal development • Determines if additional investigation warranted • Not diagnostic • Screening should have established psychometric qualities (precision, accuracy, etc.) • Easy to perform and interpret, inexpensive, and acceptable to child/parents
Surveillance and Screening • AAP recommends formal screening at 9, 18, and 24 or 30 months, and if concerns raised by parent/physician during routine surveillance • AAP also recommends all 18 month olds be screened with an autism-specific tool
Surveillance and Screening • Screening Tests: • Parents’ Evaluation of Developmental Status (PEDS) • Ages and Stages Questionnaires (ASQ) • ~15 minutes, by the parent • Generates a pass/fail score in four development domains • Infant-Toddler Checklist for Language and Communication • ~5-10 minutes, by the parent • Identifies scores 1.25 SD below normal • Brigance Screens-II
Surveillance and Screening • Screening Tests • Bayley Infant Neurodevelopmental Screener Test • Direct examination • Scores identify high, moderate, and low risk for DD • Denver Developmental Screening Test-II (DDST-II) • Direst examination • Identifies risk category: normal, questionable, abnormal
Surveillance and Screening • Screening Tests (Behavioral) • Children with undetected DD often present with behavioral issues • Eyberg Child Behavior Inventory/Sutter-Eyberg Student Behavior Inventory • Pediatric Symptom Checklist (PSC) • Parents’ Evaluation of Developmental Status (PEDS) • Ages and Stages Questionnaires: Social Emotional (ASQ:SE) • Brief Infant-Toddler Social-Emotional Assessment (BITSEA) • Conners Rating Scale-Revised Long Form (CRS-R) • Modified Checklist for Autism in Toddlers (M-CHAT) • Vanderbilt ADHD Parent Rating Scale (VADPRS)
Surveillance and Screening • Outcomes of screening • Normal development and few psychosocial risks—continue routine care • Low-Average development and psychosocial risks , but pass screening—close surveillance • Failing a screening test—these children need additional assessment/evaluation • Referral for diagnostic evaluation/early intervention services • Results of parent-completed tool are adequate for referral
Evaluation and Diagnosis • Developmental intervention • Children 0-36 months—agencies (usually state run, i.e. Early Steps) determine if children with suspected/diagnosed DD qualify for services • Multidisciplinary • Speech and Language Pathologist • Occupational and Physical Therapy • Social Worker • Psychological evaluation if needed • Focus on need for services rather than diagnosis
Evaluation and Diagnosis • Developmental intervention • Children 3-5 years—preschool special education services are available (i.e. Headstart) • Continued services—may be in or out of classroom • Children older than 5 years—referrals usually made through public school system • Private evaluations/services are also available
Evaluation and Diagnosis • Children who fail developmental screening may need further medical evaluation • Evaluation for iron deficiency anemia • Evaluation for lead poisoning (if risk factors for lead poisoning present) • Formal hearing testing (BAER) • Vision testing (full ophthalmologic exam) • Thyroid function testing (if no NBS, or signs of thyroid disease) • Metabolic screening (if abnormal or no NBS) • Neuroimaging (MRI vs CT)
Evaluation and Diagnosis • Children who fail developmental screening may need further medical evaluation • Chromosomal/Cytogenetic Testing (if +family history) • Down Syndrome (karyotype), Fragile X (FMR1), Rett Syndrome(MECP2), Prader-Willi/Angelman (FISH) • EEG if suspected seizure activity/encephalopathy (Landau-Kleffner) • CPK/Aldolase if abnormal muscle tone (Muscular dystrophy)
Other diagnoses • MentalRetardation (MR)—a state of functioning beginning in childhood characterized by limitations in intelligence and adaptive skills • DSM-IV Criteria for MR: • Significant sub-average intellectual functioning • Adaptive functioning deficit or impairment • Onset before 18 years of age • Cognitive impairment requires IQ testing (accurate for ages ≥5 years) • Mild—50 to 70 IQ ( 70 is 2 SD from normal—100) • Moderate—40 to 50 • Severe—20 to 40 • Profound—<20
Other diagnoses • Adaptive skills—skills of daily living needed to live, work, and play in the community • Communication, social skills, self-care, home living, reading, writing, mathematics, work, leisure, health and safety • Considered impaired when there is a deficit in two or more areas • American Association on Mental Retardation (AAMR) also has a similar definition of MR, but also describes supports needed (intermittent, limited, extensive, or pervasive) • The terms GDD and MR are not interchangeable
Other diagnoses • Prevalence of MR in general population is 1-3% • Intellectual testing • Weschler Preschool and Primary Scale of Intelligence (WPPSI) • Weschler Intelligence Scales for Children (WISC-III) • Stanford-Binet Intelligence Scale • Kaufman Assessment Battery for Children • McCarthy Scales of Children’s Abilities • Differential Ability Scales • Leiter International Performance Scales
Other diagnoses • Adaptive Testing • Vineland Adaptive Behavior Scales • AAMR Adaptive Behavior Scales • Woodcock-Johnson Scales of Independent Behavior
Other diagnoses • Prognosis for MR—dependent on severity: • Mild—can be taught to read/write, live independently and hold jobs as adults • Moderate—probably will not learn to read/write, but may live/work in semi-independent supervised settings • Severe/profound—require substantial lifelong support • Also dependent on etiology of MR and co-morbid conditions
Autism Spectrum Disorders (ASD) Neurodevelopmental disorders characterized by impairments in three domains: Socialization Communication Behavior Includes: Autistic disorder Asperger disorder Rhett’s disorder Childhood Disintegrating disorder Pervasive developmental disorder, not otherwise specified (PDD-NOS) Other diagnoses
Other diagnoses • Autism Spectrum Disorders • Occurs in ~1 in 150 to 1 in 500 children • Increasing incidence since 1970s—due to increased awareness/changes in case definition • MR /seizures common • Pathogenesis incompletely understood • Overwhelming evidence does not support association with immunizations and autism
Other diagnoses Autistic disorder—DSM-IV Criteria: • A total of six (or more) items from (1), (2), and (3), with at least two from (1), and one each from (2) and (3): • Qualitative impairment in social interaction, as manifested by at least two of the following: • Marked impairment in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction • Failure to develop peer relationships appropriate to developmental level • A lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (eg, by a lack of showing, bringing, or pointing out objects of interest) • Lack of social or emotional reciprocity
Other diagnoses • Qualitative impairments in communication as manifested by at least one of the following: • Delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gesture or mime) • In individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others • Stereotyped and repetitive use of language or idiosyncratic language • Lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level
Other diagnoses • Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following: • Encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus • Apparently inflexible adherence to specific, nonfunctional routines or rituals • Stereotyped and repetitive motor mannerisms (eg, hand or finger flapping or twisting, or complex whole-body movements) • Persistent preoccupation with parts of objects
Other diagnoses • Delays or abnormal functioning in at least one of the following areas, with onset before 3 years old: (1) social interaction, (2) language as used in social communication, or (3) symbolic or imaginative play. • The disturbance is not better accounted for by Rett's Disorder or childhood disintegrative disorder.
Other diagnoses • Diagnosis of Autism is a clinical one • Use DSM-IV Criteria • Sometimes referral to ASD specialists for definitive diagnosis • Diagnostic tools available: • Autism Behavior Checklist (ABC) • Gilliam Autism Rating Scale (GARS) • Autism Diagnostic Interview-Revised (ADI-R) • Childhood Autism Rating Scales (CARS) • Autism Diagnostic Observation Schedule-Generic (ADOS-G)
Other diagnoses • Aspergerdisorder—similar to autism • No clinical significant delays in language • Higher levels of cognitive function • Greater interest in interpersonal social activity • Specific DSM-IV Criteria for diagnosis • PDD-NOS—used for individuals with some, but not all, of the DSM-IV criteria for autistic disorder
Other diagnoses • Rhett Syndrome • Almost exclusively females • Develop normally initially, then gradually loose speech, purposeful hand use after 18 months of age • Deceleration in head growth • Mutations in MECP2 gene • Childhood disintegrating disorder • Regression in multiple areas of functioning after two years of normal development
References American Academy of Pediatrics, Committee on Children with Disabilities: Developmental Surveillance and Screening of Infants and Young Children. Pediatrics 2001; Vol 108: No.1: pp192-195. American Academy of Pediatrics , Committee on Children with Disabilities : Identification and Evaluation of Children with Autism Spectrum Disorders. Pediatrics 2007; Vol 120: No.5: pp1183-1215. Augustyn M., Clinical features of autism spectrum disorders. www.uptodate.com. Augustyn M., Diagnosis of autism spectrum disorders. www.uptodate.com. Feldman H., Developmental-Behavioral Pediatrics. Ed. Zitelli B., Atlas of Pediatric Physical Diagnosis. 2002: pp58-86. LaRosa A., Glascoe F., Developmental surveillance and screening in primary care www.uptoddate.com. LaRosa A., Glascoe F., Developmental and behavioral screening tests in primary care www.uptoddate.com. Shevell M, Ashwal S, Donley D, et al. Practice parameter: Evaluation of the child with global developmental delay—report of the Quality Standards Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology. 2003;60 :367 –380.