The Use of Thiazide Diuretics in Preventing Osteoporotic Fractures
The Use of Thiazide Diuretics in Preventing Osteoporotic Fractures. Jace Erwin BS, Michael Tilley MD, Alexandra Brown MS PRVM 868 Biomedical Informatics Driven Clinical Research Tuesday, December 4th, 2018. Background.

The Use of Thiazide Diuretics in Preventing Osteoporotic Fractures
E N D
Presentation Transcript
The Use of Thiazide Diuretics in Preventing Osteoporotic Fractures Jace Erwin BS, Michael Tilley MD, Alexandra Brown MS PRVM 868 Biomedical Informatics Driven Clinical Research Tuesday, December 4th, 2018
Background • In the past decade, antihypertensive medications have been receiving attention as potential protective treatments against osteoporotic fractures • Several observational studies have been conducted and have yielded positive, yet differing results • Long-term use of thiazides is protective rather than the current use (Kruse et al., 2015). • Use of thiazide diuretics, regardless of duration, was associated with decreased osteoporotic fracture rate (Bokrantzet al., 2016) • ALLHAT trial discovered that thiazide diuretic exposure may play a role in protecting against hip and pelvic fractures. (Puttnamet al., 2017)
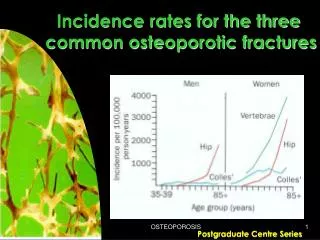
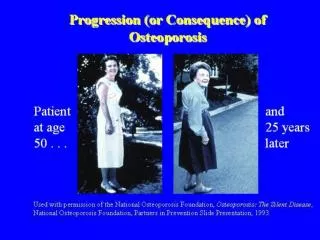
Osteoporosis • Osteoporosis, or porous bone, is a disease characterized by low bone mass and structural deterioration of bone tissue. • Leads to bone fragility and an increased risk of fractures of: • Hip • Including pelvis and proximal femur • Spine • Wrist • In the United States, more than 53 million people already have osteoporosis or are at high risk due to low bone mass (osteopenia). https://www.bones.nih.gov/health-info/bone/osteoporosis/overview
Osteoporosis T score - amount of bone you have compared with a young adult of the same gender with peak bone mass. -1 and above is considered normal. -1.1 and -2.4 is classified as osteopenia -2.5 and below is defined as osteoporosis. The T score is used to estimate your risk of developing a fracture and also to determine if treatment is required. https://pharmacypedia.org/can-vitamin-d-help-osteoporosis/
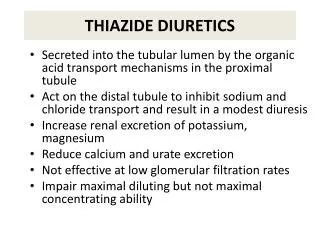
Thiazide Diuretic • Primary treatment for HTN • Mechanism of Action: Inhibit NaCl reabsorption in the distal convoluted tubule (DCT) • Drives Ca2+ reabsorption • Adverse Effects: • Hypokalemic Metabolic Alkalosis • Hyponatremia • Hyper -glycemia, -lipidemia, -uricemia, -calcemia First Aid USMLE 2016 Step 1
Possible Mechanisms • Decreased renal clearance of of Ca2+ ions (De Vecchiset al, 2017) • Stimulation of bone mineral formation (Bokrantzet al., 2016) • Osteoblast stimulation and differentiation (Lin et al, 2017) • Modulation of hypertension (Lin et al, 2017)
Central Hypothesis and Objectives • Hypothesis: Antihypertensive medications, specifically thiazides, reduce fragility fracture in patients with osteoporosis or osteopenia. • Objectives: • Characterize the population of patients with Osteoporosis who were exposed to either a thiazide diuretic or lisinopril • Assess risk of osteoporotic fracture in patients exposed to a thiazide diuretic. • Assess risk of osteoporotic fracture in patients exposed to lisinopril
Study Design • Retrospective Cohort • Inclusion: • Patients with Osteoporosis or Osteopenia defined by ICD codes AND • Documented Surescripts data for Thiazide diuretic or Lisinopril • For patients who experienced fracture, medication exposure needed to occur prior to fracture • Exclusion: • Age < 20 • Malignant neoplasm of: • Breast • Lung • Bone • Prostate
“Shopping Cart” • Demographics • Gender • BMI • Race • Vital Status • Smoking Tobacco • Smoking Tobacco Use • Years of Tobacco Usage • Smoking Quite Date • Fractures: • Proximal Femur • Pelvis • Vertebral / Spine • Distal Radius / Ulna
Methods • EMR data from KUMC patients retrospectively identified using i2b2-based data repository (HERON) • Data cleaning and organization using SQL-Lite • Statistical analysis performed in SAS version 9.4 • Chi-square / Relative Risk • Logistic Regression Modeling
7,124 with osteoporosis or osteopenia AND a documented Surescripts exposure to Thiazide/Lisinopril Removed 774 who did not meet Surescripts requirement of “claim” or “fill” 6350 remaining patients Removed 409 who had exposure to medication after fracture 5,941 patients meeting study inclusion criteria 861 patients exposed to both 2046 patients with Thiazide exposure only 3034 patients with Lisinopril exposure only
Objective 1 Characterize the Study Population • 5941 patients available for analysis • Female= 5000 | M= 941 • Typical ratio of F:M with osteoporosis is about 5 to 1 so this approximates a normal gender distribution • Average age = 71 • 7.29 % experienced a fracture (n= 433) • Medication exposure: • 34.44 % exposed to Thiazide only (n= 2046) • 51.07 % exposed to Lisinopril only (n= 3034) • 14.49 % exposed to both medications (n= 861) https://www.cdc.gov/nchs/data/hestat/osteoporsis/osteoporosis2005_2010.pdf
Objective 2 Fracture Risk - Thiazide • Thiazide Exposure • 2046 patients exposed • 136 experienced a fracture • Chi2 = 0.61; p > 0.05 at 0.4336 • RR = 0.921 [CI] crosses 1.
Objective 3 Fracture Risk - Lisinopril • Lisinopril Exposure • 3034 patients exposed • 219 experienced a fracture • RR = 1.09 [CI] crosses 1.
Objective 2/3 Compare Fracture Risk • Multiple Logistic Regression • Dependent variable= Fracture • Modeled against: • Thiazide exposure • Lisinopril exposure • OR of 1.399 with a 95% [CI]: 1.05 – 1.87, p= 0.0234 • When accounting for age, gender, ethnicity, smoking status, and BMI the OR increased slightly to 1.434 and remained significant
Conclusions • Excluding persons who were exposed to both medications then there was no association between either medication and fragility fracture. • However, when accounting for lisinopril exposure the odds of experiencing a fracture in patients not exposed to a thiazide diuretic was 1.4 times the odds of those who were exposed. (OR of 1.399 with a 95% [CI]: 1.05 – 1.87, p= 0.0234)
Strengths • Large sample size • Specific inclusion criteria Limitations • Observational study • Can not account for patients who may not have followed with KU for a fracture • EPIC data (assumption it is correct) • Possible med exposure that has not been documented • Definition for medication exposure • Relying on Surescripts claims • Potential confounders
Future Directions • I would like to rerun my own data and account for more confounding variables including: • Bisphosphonates, Prior Falls, Alcohol, CKD • I would also like to look at time of exposure to analyze dose response. • Randomized prospective studies done that can further delineate an association between antihypertensives and fracture risk
Acknowledgements • Dr. Russ Waitman, Maren Lowrance, and the entire HERON team at KUMC • University of Kansas Clinical and Translational Science Awards (CTSA) • # UL1TR002366 • # TL1TR002368 • Emily Newbold for SQL code review, as well as, the rest of my classmates for constructive feedback.
Resources • Bokrantz, T., Ljungman, C., Kahan, T., Boström, K. B., Hasselström, J., Hjerpe, P., . . . Manhem, K. (2017). Thiazide diuretics and the risk of osteoporotic fractures in hypertensive patients. Results from the Swedish Primary Care Cardiovascular Database. Journal of Hypertension, 35(1), 188-197. doi:10.1097/hjh.0000000000001124 • De Vecchis, R., Ariano, C., Di Biase, G., & Noutsias, M. (2017). Thiazides and Osteoporotic Spinal Fractures: A Suspected Linkage Investigated by Means of a Two-Center, Case-Control Study. J Clin Med Res, 9(11), 943-949. doi:10.14740/jocmr3193w • Kruse, C., Eiken, P., & Vestergaard, P. (2016). Continuous and long-term treatment is more important than dosage for the protective effect of thiazide use on bone metabolism and fracture risk. J Intern Med, 279(1), 110-122. doi:10.1111/joim.12397 • Lin, S. M., Yang, S. H., Cheng, H. Y., Liang, C. C., & Huang, H. K. (2017). Thiazide diuretics and the risk of hip fracture after stroke: a population-based propensity-matched cohort study using Taiwan's National Health Insurance Research Database. BMJ Open, 7(9), e016992. doi:10.1136/bmjopen-2017-016992 • Puttnam, R., Davis, B. R., Pressel, S. L., & et al. (2017). Association of 3 different antihypertensive medications with hip and pelvic fracture risk in older adults: Secondary analysis of a randomized clinical trial. JAMA Internal Medicine, 177(1), 67-76. doi:10.1001/jamainternmed.2016.6821 • Expressing observations from electronic medical record flowsheets in an i2b2 based clinical data repository to support research and quality improvement.Waitman LR1, Warren JJ, Manos EL, Connolly DW.AMIA AnnuSymp Proc. 2011;2011:1454-63. Epub 2011 Oct 22. • Serving the enterprise and beyond with informatics for integrating biology and the bedside (i2b2). Murphy SN, Weber G, Mendis M, Gainer V, Chueh HC, Churchill S, Kohane I.J Am Med Inform Assoc. 2010 Mar-Apr;17(2):124-30. doi: 10.1136/jamia.2009.000893.