Download
1 / 49
500 likes | 1.33k Vues
NSAID Nephropathy and COX-2 Inhibitors. Kellie A Goldsborough, MD Resident Grand Rounds November 2, 1999. Case Presentation. HPI- JS is a 69 yo bm, presents to the ER with a 2 week history of nausea, anorexia, and confusion. He was given Indomethacin 19 days earlier for a gout exacerbation

E N D
NSAID Nephropathy and COX-2 Inhibitors Kellie A Goldsborough, MD Resident Grand Rounds November 2, 1999
Case Presentation • HPI- JS is a 69 yo bm, presents to the ER with a 2 week history of nausea, anorexia, and confusion. He was given Indomethacin 19 days earlier for a gout exacerbation • PMHX- Dilated cardiomyopathy, EF 20-25%, hx of alcohol abuse, hypertension, gout • MEDS- • Lotensin 20 mg q day • Digoxin 0.125mg q day • Lasix 40mg q day • K-Dur 20meq q day • Indomethacin 25mg TID x 19days
Case Presentation - cont. • All- NKDA • SH- no tobacco, no current ETOH • PE- 98.2 79 110/79 16 97% on RA • gen-thin bm, NAD, slow to respond • HEENT- PERRLA, EOMI • neck- no bruits or JVD • lungs- CTAB • heart- RRR, no M/G/R • abd- benign • ext-no C/C/E • neuro- overall depressed MS but nonfocal
Case Presentation - cont • Labs were significant for a BUN/crt of 147/4.7 (had been 13/1.1 19 days earlier) • Admitted, NSAID and ACE were discontinued • Negative UA, U/S, and duplex • Renal function improved, ACE was restarted, he was discharged 4 days later with BUN/crt of 54/1.0, advised against NSAIDS • Didn’t follow up, returned to the ER 22 days later, admitted to taking a “pain med”, his BUN/crt were 230/18.7 • Negative SPEP/UPEP, ANCA, anti GBM • Consistent with NSAID nephropathy • Required MICU, hemodialysis, renal function did recover, discharged to a NH 11 days later with BUN /crt of 4/0.7
Case Presentation- Clinical Questions • Why did this happen? • Could it have been predicted or avoided? • Would the substitution of a different NSAID or a COX-2 inhibitor produce any less risk for this kind of NSAID nephropathy?
Introduction • 1-5% of patients exposed to NSAIDS develop some kind of a nephropathy • NSAIDS have an extensive use profile • Estimate renal abnormality in 500,000 - 2.5 mil US citizens per year who use NSAIDS • Use is increasing due to aging, OTC availability, and advent of COX-2 inhibitors
Types ofNSAID Nephropathy • Abnormalities in sodium, water and potassium homeostasis • Vasomotor acute renal failure* • Nephrotic Syndrome • Interstitial Nephritis • Chronic renal failure most often due to papillary necrosis (acute or chronic)
Objectives of Presentation • Discuss the pathophysiology of the different forms of NSAID nephropathy focusing on the vasomotor ARF • Outline the risk factors for the development of ARF with NSAIDS • Discuss the differences between the traditional NSAIDS and the COX-2 inhibitors with regard to nephropathy
Interstitial Nephritis • Difficult to estimate, less predictable and specific, related to other medicines, ie. beta lactams • Mechanism is unclear • delayed hypersensitivity response to the NSAID • inhibition of PG synthesis leads to increased proinflammatory substances • Patients afflicted are elderly, female, on NSAIDS for months • Clinical Presentation- heavy proteinuria, RBC &WBC in micro low FENa • Treatment- withdraw the NSAID, supportive care, steroids are debated, resolution weeks to months, chronic failure or ESRD can result (75%)
Nephrotic Syndrome • Approximately 10%-12% of patients who develop renal lesions on NSAIDS have minimal change nephrotic syndrome. • Patients are female, taking NSAIDS for months • Clinical presentation- nephrotic syndrome- heavy proteinuria, edema, low albumin, etc • Microscopic specimen- fusion of the epithelial cell foot processes • Treatment- withdraw NSAID, supportive, steroids more favored
Renal Papillary Necrosis • Least common, most serious, usually results in ESRD • Seen in massive NSAID o/d in a dehydrated patient • Acute • dehydration and massive NSAID ingestion elevated toxic metabolites and vasoconstriction necrosis • Chronic • also known as analgesic nephropathy • present in 2% of the HD population • repetitive daily ingestion producing a syndrome of chronic renal failure, most often linked to phenacetin
Pathophysiology of Vasomotor Acute Renal Failure • Most common, predictable nephropathy • directly related to prostaglandin synthesis suppression in the kidney • Prostaglandins- • unsaturated FA compounds derived from arachidonic acid • formation catalyzed by cyclooxygenase (COX) 2 isoforms (COX-1 and COX-2) • function as local hormones or autocoids
Risk Factors • Mechanism is well established • Any state which results in a decreased effective arterial blood volume • congestive heart failure • cirrhosis • nephrotic syndrome • sepsis/hemorrhage/hypotension/diuretic
Risk Factors - cont • Chronic Renal Failure • prostaglandins play an adaptive role • Elderly • decreased GFR, vasculature less responsive, decreased protein binding and decreased hepatic metabolism of drug
Are All NSAIDS Created Equal?Sulindac • Bunning et al, 1984 • case report of 3 patients who developed ARF on traditional NSAIDS, but no adverse renal effects on sulindac • concluded that sulindac had less renal toxicity • sulindac is prodrug, converted to active form then converted to a sulfone which is inactive as a prostaglandin inhibitor
Mistry et al • More controlled study of sulindac • 9 patients, ages 35-45 • CRI with creatinine clearance of 25-55 ml/min, HTN • Exclusion criteria: CHF, GI d/o, bleeding • all treated with sulindac 200 mg BID x 9days • End Points: creatinine, clearance, GFR RPF, urinary prostaglandins • Men were excluded from urinary PG measurements
Mistry et al - cont. • RESULTS: • statistically significant fall in crt clearance (p<0.02) and rise in creatinine (p<0.02) with tx • prostaglandin production was decreased but not significantly (47.2 ng/h to 35 ng/h with wide CI’s) • CONCLUSIONS: • renal impairment with HTN more susceptible to kidney dysfunction • In this population, sulindac affects renal function only marginally, has advantages over other NSAIDS
Mistry et al - cont. • Weaknesses • small study, only 9 days of treatment • urinary prostaglandins measured in only 5 patients • no comparison group • are changes really clinically significant? • creatinine change from 2.2 to 2.4 mg/dL • clearance change from 37 to 34 ml/min/m2
Whelton et al - sulindac • Prospectively randomized, triple crossover study • 12 women with chronic renal insufficiency (creatinine 1.5-3.1 mg/dL) • randomized to treatment for 11 days with ibuprofen, piroxicam, and sulindac • Endpoints: creatinine, RPF, GFR, urinary prostaglandin levels
Whelton et al - sulindac - cont • RESULTS: • Ibuprofen withdrawn on day 8 because of increased creatinine in 2 pts and hyperkalemia in 1 • There was a significant increase in creatinine level with sulindac tx (p<0.05) • Suppression of urinary prostaglandin activity was observed for all three groups • CONCLUSIONS: • cautioned the extrapolation that sulindac was renal sparing
Whelton et al - sulindac - cont • CONCLUSIONS-cont • Worse renal function and longer therapy could be responsible • ID’d creatinine of 2 mg/dL to be cutoff, also recommend renal function check at 7 days • WEAKNESSES • small study of women, no placebo group • pts who stopped ibuprofen not reflected in the final data
Eriksson et al • Randomized, double blind, crossover design • 9 patients with rheumatologic disease and renal insufficiency (mean clearance 53ml/min) • randomized to tx with sulindac or naproxen with a placebo washout period • Followed e’lytes, urine volume, crt, GFR, RPF, urinary 6 keto PGF1
Eriksson et al - cont • RESULTS: • Treatment with naproxen significantly decreased the excretion of 6 keto PGF1 while sulindac had no such effect • naproxen caused a decrease in GFR and RPF while sulindac did not • There was no change in creatinine with either treatment
Eriksson et al - cont. • CONCLUSIONS: • short term treatment with sulindac doesn’t suppress surrogate end points like naproxen does • WEAKNESSES: • 9 pts, treatment period only 7 days • 7 days of washout may not have been enough
COX-2 inhibitors - intro • COX exists in 2 isoforms (COX-1 & COX-2) • COX-1 “constitutive” • producing thromboxane, PGE2 in the kidney, prostacyclin (anti-thrombogenic and cytoprotective) • COX-2 “inducible” • turned on by inflammatory stimuli
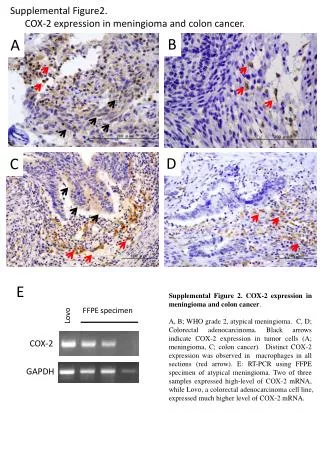
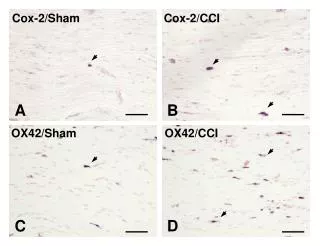
COX-2 Inhibitors • Komhoff et al in 1997 • Localized expression of COX-2 immunoreactive protein to endothelial and smooth muscle cells of vasculature in the human kidney • Does presence indicate a vital role?
COX-2 Inhibitors - cont • Table 5 Influence on COX-1 and COX-2 activity of guinea-pig peritoneal macrophages for different NSAIDS • NSAID COX-1 IC50(mmol/L) COX-2 IC50 (mmol/L) Ratio • Flurbiprofen 15 4760 317 • Indomethacin 0.21 6.4 30 • Piroxicam 5.3 175 33 • Meloxicam 5.8 1.9 0.33 • SC-236 17.8 0.01 0.00056
Stichtenoth et al • Randomized, crossover design comparing indomethacin and meloxicam • 14 women, healthy • exclusion criteria basically any diseases • randomized to meloxicam x 6 days or indomethacin x 3 days crossover with 5 day washout • Endpoints: urinary excretion of PGE2 and PGE-M
Stichtenoth et al - cont • RESULTS • Reduction of PGE2 by 43% (p<0.05) and a reduction in PGE-M by 36%(p<0.001) with indomethacin compared to baseline • Reduction of PGE2 by 13% (ns) and PGE-M by 22%(p<0.05) with meloxicam compared to baseline • Indomethacin and meloxicam significantly different when looking at PGE2 excretion
Stichtenoth et al - cont • CONCLUSIONS: • PGE2 excretion, reflecting PG production was not inhibited by meloxicam while indomethacin caused pronounced suppression • WEAKNESSES: • women only, no placebo group • measured surrogate endpoint only
Bevis et al • Open label, multicenter study • 25 pts with arthritic disease and renal insufficiency (crt clearance 25-60ml/min) • Exclusion criteria: severe disease, ulcers, hemodialysis, lithium, ACE, abnml labs • washout for 4 days, then tx with meloxicam for 28 days • Endpoints: creatinine clearance, creatinine and elytes at 14, 21, 28, 35 days
Bevis et al - cont • RESULTS: • No significant difference in the mean creatinine clearance from baseline at any time • No rise in the BUN, creatinine or K levels throughout study • CONCLUSIONS: • COX-2 selective inhibitors have minimal renal adverse effects
Bevis et al - cont • WEAKNESSES: • They didn’t measure urinary prostaglandins which appears to be a good surrogate marker for renal dysfunction • No placebo group, or comparison drug • What about studies in the other people at risk from certain disease states?
Bosch-Marcĕ et al • Randomized study in rats, yes rats! • 22 rats with induced cirrhosis and ascites • Randomized to supratherapeutic ketorolac and SC-236 (highly selective COX-2) • Multiple endpoints: urine volume, GFR, RPF, urinary PG’s
Bosch-Marce et al - cont • RESULTS: • Ketorolac resulted in significant decreases in urine volume, GFR, RPF, and PG’s when compared to baseline, SC-236 tx did not • Assay found constitutive expression of COX-2 • CONCLUSION: • Although rats with cirrhosis and ascites showed constitutive COX-2 mRNA expression, selective inhibition was devoid of any significant effect on renal function
Whelton et al - elderly • Single center, single blind, randomized, crossover study- not published yet • 29 healthy elderly with GFR 67-127 ml/min • Randomized to celecoxib or naproxen for 10 days, then crossover with a 7 day washout • Endpoints: creatinine, GFR, urinary PGE2 and 6 keto PGF1
Whelton et al - elderly - cont • RESULTS: • Significant reduction in GFR with naproxen (-7.53ml/min) as compared to celecoxib (-1.11ml/min) (p=0.004) • PGE2 significantly reduced with both naproxen (by 76%) and celecoxib (by 65%) from baseline • 6 keto PGF1 reduced to undetectable levels with both treatments
Whelton et al - elderly - cont • CONCLUSIONS: • Celecoxib does reduce urinary prostaglandins but doesn’t affect GFR in healthy elderly adults • WEAKNESSES: • The patients didn’t have very significant renal dysfunction • No placebo group, funded by drug company
Whelton et al - CRI • Multicenter, double blind, randomized, placebo controlled parallel group study • 75 pts with CRI (GFR 40-60 ml/min, and creatinine of 1.3-3.0 mg/dL) • Randomized to celecoxib, naproxen, or placebo x 7 days after washout • Endpoints: GFR, urinary PGE2 and 6 keto PGF1
Whelton et al - CRI - cont • RESULTS: • There were no significant differences in GFR between treatment groups • Both active agents reduced urinary PG’s • PGE2 by 88% with naproxen, 47% with celecoxib; 6 keto PGF1 by 82% and 48% but there was no statistical significance between groups
COX-2 Inhibitors - cont • These studies demonstrate decrease in urinary PG’s , but no change in GFR or creatinine • Is there any demonstration of renal dysfunction related to these medicines?
Local Case Series of COX-2 related nephropathies - Deterding • CASE 1- 65 yo wf with CML (dx 3/98), DM, HTN and previous episode of ARF thought to be due to TLS with resolution, baseline BUN/crt of 23/1.2. Started on Vioxx on 8/13, presented to the ER on 8/20 with a BUN/crt of 106/8.8. Also on accupril and lasix but had been for years. Work up included a negative urinalysis, ultrasound and duplex. The Vioxx and ACE were dc’d, her renal failure resolved. She was discharged 4 days later, BUN/crt of 26/0.9.
Case Series - cont • CASE 2 - 72 yo wf with obesity, DM, and chronic venous insufficiency, prolonged hospitalization (5/28-6/17) for ?PE, pneumonia and bacteremia, improved with treatment. Started on lasix on 6/7, an ace on 6/9, then on celecoxib on 6/12. Labs on 6/16 showed nml renal function. Transferred to the TCU, next lab check on 6/23, BUN/crt of 25/2.9, then 29/3.6 on 6/25, and 29/3.9 on 6/26. The celecoxib and Ace were dc’d, work up = negative ultrasound and duplex, UA showed 1-5 WBC and few bacteria. Renal function improved after stopping the celecoxib, on 10/7 it was 17/1.0.
Case Series - cont • Cases are very suggestive for COX-2 related nephropathy • Only a case series • Other variables involved, most notably the Ace Inhibitor and the diuretic tx • Other studies are needed for verification of COX-2 related nephropathies
Bottom Lines • NSAID nephropathy is a significant health issue, prevalence may increase in the future due to aging of the population, increased availability, and the new COX-2 inhibitors. • Vasomotor acute renal failure is the most common and predictable NSAID nephropathy and also the most easily avoided by careful administration of NSAIDS. • Risk factors for acute renal failure related to NSAIDS are: volume depletion, congestive heart failure, cirrhosis, nephrotic syndrome, chronic renal insufficiency and advanced age.
Bottom Lines - cont • .When looking at traditional NSAIDS, sulindac may pose less of a risk for ARF if used for a short course. • .The COX-2 enzyme is constitutively expressed in the kidney, and COX-2 inhibitors, initially promising, appear to cause inhibition of prostaglandin synthesis and limited demonstration of acute renal dysfunction. However, this may be to a lesser degree than traditional NSAIDS, more studies are needed to delineate. • .No NSAID can be regarded as completely renal sparing, we must use these medicines more judiciously with careful monitoring of renal function in those who are at risk.
Acknowledgements • Richard Appel, MD helping pick articles • Liz Deterding, MD giving me cases • Christine Brandon-Bingham • Andrew Namen, MD , Todd Hulgan, MD , Linda Lee, MD for critiquing my work