Download
1 / 52
570 likes | 1.43k Vues
The Anterior Cruciate Ligament: Injury Prevention and Treatment. Charles Ruotolo, MD FAAOS Chairman, Dept. of Orthopedics Nassau University Medical Center. Anatomy. Anteromedial bundle Smaller, tight in flexion Posterolateral bundle Larger, tight in extension

E N D
The Anterior Cruciate Ligament:Injury Prevention and Treatment Charles Ruotolo, MD FAAOS Chairman, Dept. of Orthopedics Nassau University Medical Center
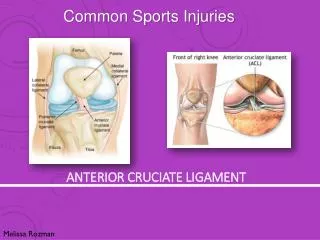
Anatomy • Anteromedial bundle • Smaller, tight in flexion • Posterolateral bundle • Larger, tight in extension • Both bundles parallel in extension • In flexion posterolateral insertion moves forward • Bundles cross in flexion • Posterolateral bundle loosens
Anatomy of the ACL • Innervated by the tibial nerve • Has golgi tendon receptors • Torn ACL knees have altered proprioception with delayed reflex hamstring latency • Middle geniculate artery
Incidence of ACL tears • Incidence quantifies the occurrence of new cases of a given injury in a population • The incidence in the USA is 200,000 annual ACL tears
Incident Rate • The rate at which an incident occurs • Can be reported as the number of new injuries per athlete exposures or athlete hours
ACL Incidence and Incident rate • Incidence is higher in men than women • In certain sports the incident rate is higher in women than men • Rate 1.5-4.6 Times higher for females than males
ACL Tears in Females Anatomical and Hormonal Factors 1. Intercondylar notch size. The size and shape of the notch tends to be smaller in women.
ACL Tears in Females • Anatomical and Hormonal Factors2. Pelvis size. Women typically have a wider pelvis3. Ligament laxity. Women's ligaments can be more lax than men's ligaments. • Also, research has shown that women's muscle tissue is more elastic than male muscle tissue causing excessive joint motion combined with increased flexibility • As a women approaches the end of knee extension, the femur glides forward more than in men.
ACL Tears in Females • Anatomical and Hormonal Factors4. Reflex time. It has been shown that female muscles stabilizing the knee may take a millisecond longer to respond than their male counterparts. 5. Hormones. Changes in estrogen levels during the menstrual cycle may affect the strength of the ACL.
ACL Tears in Females • Anatomical and Hormonal Factors6. Quadriceps/Hamstring Strength Ratio. • The hamstrings reduce forward motion of the tibia (tibial translation) in synergy with the ACL. "In men, the hamstring is recruited first to stabilize the knee during anterior tibial translation. On the other hand, women rely more on the quadriceps and gastrocnemius to resist anterior tibial translation." Poor hamstring strength in both sexes may be a cause for ACL injury. If the hamstring cannot balance the power of the quadriceps, then this imbalance can cause significant stress to the ACL.
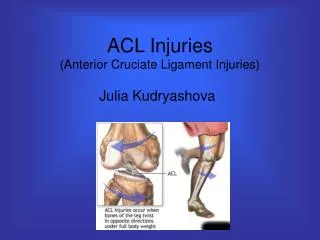
Injury Mechanism • 50-70% are noncontact injuries • These usually involve planting, cutting and jumping • This also commonly involves imbalances of body weight and malalignment of body position
Mechanisms The skier falls back, trying to pull himself up, the boot levers the knee forward in conjunction with a forceful quadriceps contraction
Mechanisms Landing from a jump
Mechanisms Sudden stop on extended knee
Mechanisms Deceleration with change of direction
ACL Tear Prevention • Mandelbaum et al, AJSM 2005 • Neuromuscular and Proprioceptive Training program • Prospective nonrandomized 1041 female soccer players • 1905 in control group • 88% decrease in ACL in year 1 and 74% in ACL injury in year 2
ACL Tear Prevention • Mandelbaum et al, AJSM 2005 • Program consisted of • Warm up: Jog line to line, shuttle run, backward running • Stretching • Strengthening: Walking lunges, Russian hamstrings, single toe raises • Plyometrics Lateral hop, Forward hop, Single leg hop, vertical jumps, scissor jumps • Agilities: shuttle run, diagonal run, bounding run
ACL Tear Prevention • Hewett et al AJSM 1999 • 6 week preseason training program of flexibility, plyometric and weight training • All HS aged soccer, volleyball, and basketball • 366 trained girls, 463 untrained girls and 434 untrained boys
ACL Tear Prevention • Hewett et al AJSM 1999 • Knee Injury rate was .43 for untrained group, .12 for trained group and .09 for male group • Noncontact rate was .35 for untrained, 0 for trained and .05 for male group • Untrained group had a 3.6 X injury rate than trained group
ACL Tear Prevention: Which Single Component Works? Yes No • Biofeedback • Isolated balance training • Isolated plyometrics • Isolated strengthening
Initial History of Injury • Noncontact injury • Audible pop • Immediate hemarthrosis • greater than70% of pts w/ acute hemarthrosis will have ACL tear
Initial Exam • Hemarthrosis • Lachman Test • Done at 20-30 degrees of knee flexion • Pivot shift Test
Lachman Test 1+ 0-5 mm of anterior displacement - sometimes with an end point 2+ 5-10 mm of anterior displacement - with no end point 3+ 10 mm of anterior displacement - with no end point Comparison to other side is important
Pivot Shift Test Most specific test for ACL deficiency - knee is placed in full extension w/ application of valgus stress & internal rotation stress; - the knee will remain reduced in full extension, will subluxate in 20-30 deg of flexion (w/ appropriate stress), and will then again reduce w/ further flexion; - at 40 deg: iliotibial band provides reduction;
Xray Findings • Segond Fracture 12% • Radiology. 1993 Jun;187(3):821-5.
Xray Findings • Lateral Femoral Condyle impaction Injury 8% • Radiology. 1993 Jun;187(3):821-5.
Xray Findings • Posterolateral Tibial Plateau Fx 44% • Radiology. 1993 Jun;187(3):821-5.
Xray Findings • Tibial Spine Avulsion Fracture 8% • Radiology. 1993 Jun;187(3):821-5.
MRI Findings • any discontinuity or signal change in the ligament is indicative of ACL tear; • indirect signs of ACL tear: • always look for signs of additional injury (meniscal tear, PCL tear, LCL tear); • Pivot shift injury: combination of signal changes in lateral femoral condyle and posteror lateral tibial plateau: • abnormal slope of ACL
Treatment Options • Surgery: Reconstruction • Restores stability, prevents further injury • >5 year OA rate 17-50% • ACL and MCL • ACL and PLC
Treatment Options • Conservative Treatment • there is no good evidence that brace wear decreases the rate of re-injury • older patients w/ isolated ligament injury who are willing to moderate their activity will find non-operative treatment to be satisfactory in the majority of cases (over 80%)
Graft Options: Autograftvs Allograft Autograft Allograft • Graft site morbidity • Infection rate • Strength • Cost
Graft Options BTB Hamstring • Graft site morbidity • Increased post op pain • Pain with kneeling • Scar length • Quad weakness • Osteoarthritis • Hamstring strength loss
Graft Options • Double bundle Hamstring graft is 2X stronger than BTB • Osteoarthritis at >5year follow up in prospective study matched for meniscal and cartilage injury • BTB 50% • Hamstring 17%
Fixation Options: Hamstring Femoral Fixation Tibial Fixation • Cross Pin Devices • Blind graft passage • Possible graft laceration • Endobutton/EZLoc/Toggle loc • Bioabsorbable screws • Bioabsorbable screws • Washerloc
Surgical Pitfalls/Complications • Harvesting complications • Tunnel Placement Single most important factor • Motion Loss • Extension: Roof impingement • Flexion: PCL impingement • Both lead to motion loss or graft laxity
Roof Impingement • line along intercondylar roof should be anterior to the line along anterior aspect of tunnel
Tibial Tunnel Howell et al, AJSM 2001 • Needs to be 65-70 degrees in the coronal plane
Tibial Tunnel • Tunnel >75 degrees had greater loss of flexion and anterior laxity • Correlates with top of gracilis, anterior MCL Cuomo et al: Arthoscopy 2006
Femoral Tunnel • Vertical Placement • Rotational instability • Anterior Placement • Leads to flexion loss or elongated graft
Femoral Tunnel • ACL graft should pull up into the tibial tunnel by about 2-3 mm with extension when fixed on the femoral side • a graft that tightens (pulls up into tibial tunnel) w/ flexion will have a much higher likelyhood of failure and usually indicates a femoral tunnel too far anterior in notch.
Femoral Tunnel • Posterior Placement • Leads to extension loss • Diminished by fixing graft in extension
Femoral Tunnel • Right knee • Graft placed at 10 oclock • Left Knee • Graft placed at 2 oclock
Post-Operative Rehab • Drop lock brace locked in extension when walking for 2-3 weeks • Goal for week 1 • Isometric quad contractions, work on full extension • Goal for week 2 • IQC, full extension, flexion to 110 degrees • Limited to 90 degrees x 2 months for meniscal repair