Download
1 / 29
320 likes | 961 Vues
Anterior Cruciate Ligament Rupture. By Sarah Hart. Learning Outcomes. To describe the background anatomy of an ACL. Describe the ACL mechanism of injury, and signs and symptoms. Explain the classification and aetiology of ACLR, concentrating on Grade III

E N D
Anterior Cruciate Ligament Rupture By Sarah Hart
Learning Outcomes • To describe the background anatomy of an ACL. • Describe the ACL mechanism of injury, and signs and symptoms. • Explain the classification and aetiology of ACLR, concentrating on Grade III • Describe the subjective, objective and further investigation into distinguishing an ACL rupture. • Treatment options - operative vs. non operative. • Explain the stages of rehabilitation and treatment protocols • How the ACL contributes in a functional task
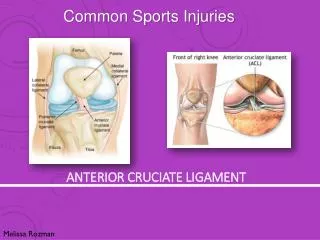
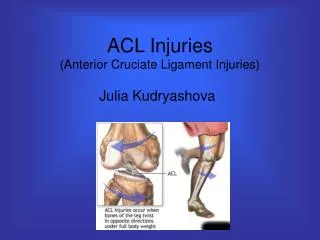
Background Anatomy • The anterior cruciate ligament is located within the joint capsule of the knee. • Approximately 31-38mm long and 10-12mm across (Odensten 1985) • Origin- anterior part of the tibial plateau, near the tibial spine. • Insertion- posteriorly on the femur at the lateral wall of the intercondylar notch Palastanga (2001). • It runs upwards and backwards from it’s origin.
Consist of 2 parts Anteromedial band- makes up 49% of the ligament. Tension occurs in this portion when the knee is flexed Posterolateral band- makes up the remain 51%. Tension occurs during extension. Intermediate band- some literature suggest there is an intermediate band which is an amalgamation of fibres from the posterolateral and anteromedial bands. (Beasley et al 2005) Role in the body The ACL provides both mechanical stability and proprioceptive feedback to the knee. Restrains anterior translation of the tibia on the femur. Prevents hyper-extension of the knee. Secondary stabilizer to valgus stress Controls rotation of the tibia on femur in the last 30 degrees of knee extension. (part of the locking mechanism) (Tortora 00) Background Continued
Mechanism of injury • An ACL injury (either grade I, II or III) can occur during the following:- • Sudden hyperextension of the knee. • Body weight twisting across the knee joint causing a shearing force while the foot is still planted on the ground. • Sudden deceleration.
Signs and symptoms • Patient will report:- • “pop” sound or sensation • Instability • Swelling • Poorly localised pain. • On some occasions ACL ruptures can occur with MCL (Medial Collateral Ligament) ruptures and medial menisci tearing. This is referred to as “unhappy triad” (Prentice 2001)
Classification of ligament injuries • Grade I- mild minimal signs and symptoms, minimal functional loss and resolves in a few days • Grade II- moderate- partial structural disruption, swollen tender, may show some signs of instability. Performance deficit for up to 6 weeks. • Grade III-severe extensive structural disruption, extensive swelling, severe pain, joint unstable. Performance deficit. Minimum 6-8 weeks> indefinitely. (Prentice 2001)
Aetiology • Ligaments are slow to heal due to their hypovascular nature. • Pathologically ligaments are a type of dense connective tissue, 90% type I collagen, 9% type III collagen and 1% fibroblast cells
Aetiology continued • Inflammatory phase • After trauma, mast cells, basophils and platelets go to the injured sit and trigger a chemical cascade. The chemical mediators from this cascade are either vascular or cellular response. There is an increase in blood toward the injured site which also means there are an increase in white blood cells count in the area, exhibiting a phagocytic response to remove debris. Which will then allow the proliferation phase to begin. (Watson 2004).
Aetiology continued • Proliferation phase • During proliferation fibroblasts and endothelial cells migrate towards the trauma site to lay down collagen and restore blood supply toward the region (angiogenesis). This create scar tissue as all fibres are laid down in a mish-mash formation. (Watson 2004)
Aetiology continued • Remodelling phase. • Basically the re-orientation of collagen fibres. In this phase there is a re-absorption of type III collagen fibres and replaced by type I collagen fibres. • The re-orientation of fibres is achieved by stressing the joint during rehabilitation. Either in physiological and/or accessory movements. • The aim of rehabilitation is for the tissue to become as similar as possible to parent tissue (Watson 2004)
Applied onset • Grade III • Subjective • Objective • Further investigations • Surgery options • Rehabilitation programmes • Different approaches
Subjective assessment • As mentioned before patient will c/o:- • Instability in the knee. • Poorly localised pain. • Swelling- cause by joint haemarthrosis. • “Pop” sound. • Hopefully the patient will be able to explain the mechanism of injury.
Objective assessment • Posture- If the patient decides not to have an operation, all joints above and below the knee need to be cleared to ensure a successful rehabilitation. • AROM- flexion, extension, medial lateral rotation. • PROM- GENTLE over press of movements
Further investigations • Anterior drawer test • Lachmans test– knee in 20-30° flexion • Valgus Stress test • If all are positive the therapist can distinguish between a grade II and grade III tear. • MRI can also indicate a rupture.
Pre-operative • There are two treatment options • However before either programme can be implemented, swelling, pain and inflammation has to subside. ROM, quadriceps and normal gait pattern has been restored. This occurs 2-3 wks post injury (Shelbourne 1991). • Non-operative- patients or surgeons may elect not to have/ carry out surgery on an ACL deficient knee. • Operative- the surgeon elects from a range of replacements.
Treatment options (Beasley et al 2005)
Post operative • Single most important rehab consideration is the initial strength of graft. • Predicted strength timescales are:- • 3 months- 57% • 6 months- 56% • 9 months- 87% • Immediately after surgery, swelling and pain must be controlled using cold compression (Beasley et al 2005)
Early stage • ROM can begin immediately. Achieving full extension is an early stage goal. • Mobilisation of patella, to prevent restriction of flexion and extension • Cardio-respiratory exercises begin from week 1 using the bike as it is a closed kinetic chain exercise that is non-weight bearing. • The patient can use crutches to stand in the first 2 weeks. The patient can come off the crutches once they are able to tolerate full weight-bearing, minimal swelling and a near normal gait. • Strengthening of surrounding structures e.g. hamstrings and quads by SLR and Quad contractions respectively
Mid stage • Progressive strengthening treatment. • Closed kinetic chain exercises- i.e. squats and lunges. Starting to incorporate some open kinetic chain movement BUT only in flexion and extension. No rotational work. • Restoring neuromuscular control- to re-establish balance and stimulate muscle and joint mechanoreceptors. • Cardio-respiratory walking on a treadmill and swimming are advocated in this period of rehabilitation. Norris (2004)
Late stage • Functional training is incorporated during all phases but is emphasised even more during the late stages. • The rehabilitation programme in this phase needs to be able to replicate the stresses and strains that are placed on the ligament by the individual but in a controlled environment. Norris, (2004).
There are different arguments as to how long a rehabilitation programme for a ACL reconstruction. Widely range protocols are:-Shelbourne and Nitz 4-6 months Andrews and Wilks 5-6 months Fu and Irrang 6-9 months Campbell Clinic 6-12 months Paulos and Stren 9 months Kerlan and Jobe 9 months. (Prentice 2001) General criteria for each programme:- No joint effusion Full ROM Isokinetic testing reveals that hamstrings and quadriceps are within 85-100% of normal strength Satisfactory ligament stability using an arthrometer Successful progression from walking to running Successful performance of functional task i.e. twisting. Different approaches
Functional task • Kicking a ball. • From the knee going to a flexed position to an extended position, during the movement. • The ACL alongside the hamstring group work together to prevent hyperextension when bringing the lower leg through into knee extension. • The ACL also prevents anterior translation of the tibia on the femur.
References • Beasley, L.S., Welland, D.E, Vidal, A.F., Chhabra,A., Herzka, A.S., Feng, M.T. and West, R.V., (2005) Anterior Cruciate Ligament Reconstruction: A Literature Review of the Anatomy, Biomechanics, Surgical Consideration, and Clinical Outcomes, Operative Techniques in Orthopaedics, 10, 5-19 • Norris, C.M., (2004), Sports Injuries Diagnosis and Management, Butterworth Heinemann, London. • Odensten M, Gillquist J, (1985) Functional Anatomy of the Anterior Cruciate Ligament and a Rationale for reconstruction, Journal of Joint Surgerery American, 67, 257-262. • Palastanga, N., et al (2001), Anatomy and Human Movement, Structure and Function, Butterworth and Heineman. • Prentice, W.E., (2001), Rehabilitation Techniques in Sports Medicine, 3rd Edition Mosby, London. • Tortora, G.J. and Grabowski, S.R., (2000), Principle of Anatomy and Physiology, John Wiley and Sons.
References • http://www.aafp.org/fpm/20050300/67atoo_f2b.gif Anterior drawer test • http://medpics.findlaw.com/imagescooked/4392W.jpg ACL ruptures 22/02/08 • http://www.electrotherapy.org/index.htm Watson 2004 • http://static.flickr.com/51/136445065_0c2a3b4de1.jpg - imflamtory response • http://images.google.co.uk/imgres?imgurl=http://www.csua.berkeley.edu/~nadeem/pictures/2003-10-23-acl/pics/kneemri.jpg&imgrefurl=http://www.csua.berkeley.edu/~nadeem/acl2.htm&h=360&w=360&sz=53&hl=en&start=54&um=1&tbnid=pjlYncdvfshGAM:&tbnh=121&tbnw=121&prev=/images%3Fq%3Dknee%2Bsurgery%2B%252B%2BMRI%26start%3D40%26ndsp%3D20%26um%3D1%26hl%3Den%26sa%3DN Background picture. Accessed 22/02/08 • http://images.google.co.uk/images?um=1&hl=en&q=anterior+cruciate+ligament&btnG=Search+Images ACL anatomy picture Accessed 22/02/08