Download
1 / 35
350 likes | 461 Vues
Measurement of invivo anterior cruciate ligament strain during dynamic jump landing 2011 .A. Taylor a, M.E.Terry c, G.M.Utturkar a, C.E.Spritzer b, R.M.Queen c, L.A.Irribarra Abstract

E N D
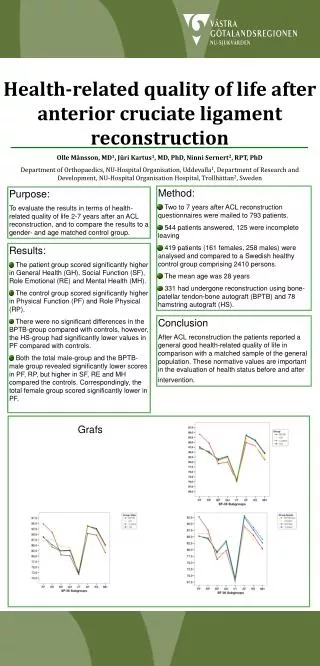
Measurement of invivo anterior cruciate ligament strain during dynamic jump landing2011 .A. Taylor a, M.E.Terry c, G.M.Utturkar a, C.E.Spritzer b, R.M.Queen c, L.A.Irribarra Abstract Despite recent attention in the literature, anterior cruciate ligament (ACL) injury mechanisms are controversial and incidence rates remain high. One explanation is limited data on in vivo ACL strain during high-risk, dynamic movements. The objective of this study was to quantify ACL strain during jump landing. Marker-based motion analysis techniques were integrated with fluoroscopic and magnetic resonance (MR) imaging techniques to measure dynamic ACL strain non-invasively.
Abstract First, eight subjects’ knees were imaged using MR. From these images, the cortical bone and ACL attachment sites of the tibia and femur were outlined to create 3D models. Subjects underwent motion analysis while jump landing using reflective markers placed directly on the skin around the knee. Next, biplanar fluoroscopic images were taken with the markers in place so that the relative positions of each marker to the underlying bone could be quantified. Numerical optimization allowed jumping kinematics to be superimposed on the knee model, thus reproducing the dynamic in vivo joint motion. ACL length, knee flexion, and ground reaction force were measured. During jump landing, average ACL strain peaked 55 +/- 14 ms (mean and 95% confidence interval) prior to ground impact, when knee flexion angles were lowest.
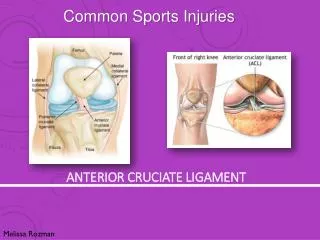
1. Introduction Over 200,000 anterior cruciate ligament (ACL) injuries occur in the United States every year, half of which are experienced by young athletes between 15 and 25 years of age (Miyasaka et al., 1991; AAOS, 2008). The consequences of ACL deficiency incurred from ACL injury include pain, instability, damage to the menisci, and early-onset osteoarthritis (OA) (Fairclough et al., 1990; Roos et al., 1995; Fithian et al., 2002; Hill et al., 2005). For these reasons, between 100,000 and 175,000 patients elect to undergo ACL reconstruction annually (Koh, 2005; Griffin et al., 2006). Although surgical intervention provides good short-term outcomes, long-term results are less consistent (Asano et al., 2002; Wolf and Lemak, 2002; Lohmander et al., 2004; von Porat et al., 2004; Grossman et al., 2005).
1. Introduction Some studies have suggested that current reconstructive techniques do not decrease the probability of developing OA when compared to non-operative treatment (Fink et al., 2001; Lohmander et al., 2004; von Porat et al., 2004; Lohmander et al., 2007; Butler et al., 2009). Kreuzbandimplantate helfen nicht bei der Verringerung der Wahrscheinlichkeit von Osteoarthritis im Vergleich zu nicht operierten Kreuzbandbehandlungen Because ACL injury affects such a young population (Roos et al., 1995; Beynnon et al., 2005) and surgery has mixed results in preventing early-onset OA (Fithian et al., 2002; Lohmander et al., 2007), there has been great interest in developing ACL injury prevention programs (Hewett et al., 1999; Heidt et al., 2000; Myklebust et al., 2003; Gilchrist et al., 2008).
Introduction However, the levels of success achieved by current prevention programs have shown varied efficacy (Hewett et al., 1999; Soderman et al., 2000; Myklebust et al., 2003; Mandelbaum et al., 2005; Pfeiffer et al., 2006; Barber- Westin et al., 2009) and despite their implementation, high rates of non-contact ACL injuries persist (Agel et al., 2005). Trainingsprogramme sind nicht unbedingt wirksam -die hohe Anzahl an „Nicht-Kontakt“ ACL Verletzungen bleibt
These findings suggest that there is an incomplete understanding of the underlying injury mechanisms. Specifically, there are limited in vivo data on ACL strain, a critical parameter for predicting ACL failure. Numerous studies have investigated ACL injury mechanisms using videographic and motion analyses (Chappell et al., 2002; Chappell et al., 2007; Krosshaug et al., 2007a, 2007b; Boden et al., 2009; Hewett et al., 2009; Nagano et al., 2009). These studies provide important kinematic data, but do not directly measure ACL strain. Many previous studies have examined ACL loading in cadavers (Draganich and Vahey, 1990; Markolf et al., 1990; Woo et al., 1991; Li et al., 1999; Kanamori et al., 2000; DeMorat et al., 2004). Although these data give valuable information on ACL function, their application to in vivo environments are restricted by an inability to recreate complex multi-planar loading conditions experienced during dynamic jumping and cutting activities.
Using implantable strain gauges, some in vivo measurements of ACL strain have also been reported (Beynnon and Fleming, 1998; Fleming et al., 1999; Cerulli et al., 2003; Fleming and Beynnon, 2004). Beynnon and Fleming et al. (Beynnon et al., 1997; Fleming et al., 1998; Fleming et al., 1999) ran a series of in vivo strain studies to understand how an ACL graft would be loaded during common post-surgical rehabilitation exercises and daily tasks. These data were the basis for many pertinent clinical rehabilitation guidelines. However, there are limited data on ACL strains during sport-specific dynamic movements. Dynamic ACL strain data are needed to accurately predict what motions predispose the ACL to injury. The objective of this study was to measure in vivo ACL strain non-invasively during a dynamic jumping activity using a novel method developed by our laboratory.
All subjects were imaged with a 3Tmagnet (Trio Tim, Siemens Medical Solutions USA, Malvern, PA). Coronal, sagittal, and axial images were taken with the patient supine and the knee in a relaxed position. Coronal…Frontalebene (blau) Axilaebene…Transversalebene (gelb) Sagittalebene (rosa) From these images, the outer margins of the cortical bone and ACL attachment site were outlined using solid- modeling software. These tracings were compiled to create subject-specific 3D models of each tested knee. The location of the ACL was confirmed using orthogonal image sets. This methodology accurately measures the location of the ACL footprint center to within 0.3 mm, as described previously (Abebe et al., 2009). Subjects next underwent a 3D motion analysis using an eight camera motion capture system with a sampling rate of 240 Hz (Motion Analysis Corporation, Santa Rosa, CA). Also, centered within the capture volume were four embedded force plates (AMTI, Boston, MA, USA) with a sampling rate of 2400 Hz
Additionally, non- symmetric clusters of markers were also placed on the thigh and shank until a total of 28 markers were positioned on the leg (Fig. 1). The primary goal of this complex marker set was to over-constrain each anatomical segment (thigh, shank) so that the effects of skin motion could be minimized via numerical optimization, as demon- strated by previous investigators (Andriacchi et al., 1998; Alexander and Andriacchi, 2001; Ngai et al., 2009; Ngai and Wimmer, 2009). Marker data were captured initially during a static standing trial with the subject’s feet shoulder width apart for one second. Next, subjects performed five successful trials of a jump landing task. Starting from a platform 0.47 m off of the ground and half their standing height away from the force plate’s edge, subjects were asked to jump from the platform onto two force plates, then immediately jump straight up with maximal effort and land back on the same force plates again.
….subjects were imaged with the markers still in the same positions using biplanar fluoroscopy (DeFrate et al., 2004; Caputo et al., 2009) …the 3D joint model was imported into the environment and viewed from two orthogonal directions corresponding to the location of the image sources of each fluoroscope. Next, the position and orientation of the model were manipulated manually in six degrees-of-freedom (6DoF) until their projections, as viewed from the two orthogonal directions, matched the outlines on the fluoroscopic images (Fig. 2).
3. Results 3.1. Validation study Linear regression demonstrated that the two techniques had excellent correlation,with a coefficient of determination of 0.92. Root mean square error between the measurements was 0.5 mm. These results indicate that the combined methodology accurately measures ACL deformation up to 45° of flexion during a quasi-static lunge.
The study showed that the peak ACL strain occurred 55+/-14 ms prior to impact when ACL length was 12 +/- 7% longer than an MRI based reference length. In the future, this system will be used to examine kinematic parameters that elevate ACL strain. After ground contact, the ACL length initially spiked to a local maximum, but quickly decreased as the knee bent. The post impact local maximum in the ACL length demonstrated local maximum in the ACL length demonstrated 5% less relative strain than the absolute maximum prior to impact. In the current study, we detected peak ACL strains 55 ms prior strains 55 ms prior to impact, when flexion angles were their lowest. This is consistent with the finding that non-contact ACL injuries most commonly occur with the knee in less than 30° of flexion. Moreover, videographic analyses of real time sports injuries have determined that a significant number of non-contact injuries are associated with a perturbation prior to contact with the ground (Olsen et al., 2004; Krosshaug et al., 2007a, 2007b; Boden et al., 2009), a time when we observed higher ACL lengths. …15–19% ultimate strain threshold range reported by Butler et al.
One limitation of the combined method is that it was unable to be validated dynamically. A second limitation is that the presented technique was only validated to measure ACL deformations accurately up to 45° of flexion. However, because most injuries occur at flexion angles less than30° (Chaudhari …. Finally, strain was approximated by normalizing ACL length to the reference length measured in a relaxed position during MR imaging, where the fibers of the ACL appeared taut. It is difficult to know precisely the reference length of the ACL in vivo since it cannot support axial compression. These data will provide valuable information for developing prevention programs aimed at reducing the incidence of ACL injury.
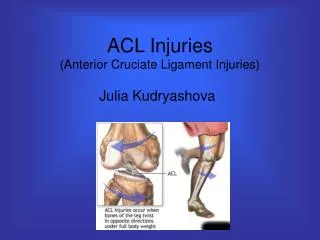
The Effects of a Valgus Collapse Knee Position on In Vivo ACL Elongation 2013 G. M. UTTURKAR There are conflicting data regarding what motions increase ACL injury risk. More specifically, the mechanical role of valgus collapse positions during ACL injury remains controversial. Our objective was to evaluate ACL …. Artikel wird/wurde detailliert besprochen und dementsprechend muss der Inhalt dieser Arbeit bei der Prüfung relativ genau gekonnt werden. Custom-written software (also known as bespoke software or tailor made software) is software that is specially developed for some specific organization or other user (Speziellfür die Anwendungprogrammierte Software). Anatomievideo Knie http://www.youtube.com/watch?v=_q-Jxj5sT0g
Perspectivearticle Hip extension, kneeflexion paradox: A newmechanismfor non-contact ACL injury Javad Hashemi a,b,n, Ryan Breighnera, NaveenChandrashekarc, Daniel M. Hardy b,g, AjitM. Chaudharid, Sandra J. Shultz e, James R. Slauterbeckf, Bruce D. Beynnon2010 Abstract …Todate, numerous non-contact ACL injurymechanismshavebeenproposed, but noneprovides a detailedpictureofsequenceofeventsleadingtoinjuryandtheexactcauseofthisinjuryremainselusive. In thisperspectivearticle, wepropose a newconceptionof non-contact ACL injurymechanismthatcomprehensivelyintegratesriskfactorsinsideand outside thekneejoint. The proposedmechanismis robust in the sense thatitisbiomechanicallyjustifiableandaddresses a numberofconfoundingissuesrelatedto ACL injury In diesem Perspektive Artikel wird ein neues Konzept des Nichtkontakts ACL Verletzungsmechanismus vorgestellt, der umfassend Risikofaktoren innerhalb und außerhalb des Kniegelenks integriert. Der vorgeschlagene Mechanismus ist in jenem Sinne robust, dass er biomechanisch zu rechtfertigen ist. Zusätzlich behandelt er einige verwirrende Fragen bezogen auf ACL Verletzungen.
In der Literatur bisher angeführte Verletzungsvorgänge ACL • anteriorshearforcemechanisms - majorcontributortotheanteriorshearforceisthecontractionofquadricepsmusclesresulting in significantanteriortibialtranslationatlowkneeflexionangles • axial compressiveloadmechanism • hyperextensionmechanism • valguscollapsemechanism — owingeitherto pure abductionofthe distal tibia relative tothefemurortotibiofemoralinternal/externalrotations • internalrotationofthetibia • combinedvalgusandanteriorshear • combinedvalgusandinternaltibialtorque • valgus and external tibial torque • valgus, anteriortibialshear, and axial torqueaboutthelongaxisofthetibia
The mechanicaland/orstructuralpropertiesofthe ACL are not consideredimportant in thesemechanismspartlybecauseitispresumed, perhapsprecipitately, thatlittlecanbedoneto alter ACL sizeandstrength. In almost all ofthe ACL injurymechanismliterature (withtheexceptionofIreland, 1999), sagittal plane hip kinematicsareignoredas a directcontributorto ACL loading. Itis also frequentlyassumedthatexcessivemuscle-generatedforcesortorquescause ACL injury, but nevertheopposite. A lack ofadequatelyprotectiveco-contractionofbothkneeand hip musclesisseldomconsideredas a causeof ACL injury, despitebeingmore plausible. Es wird auch häufig angenommen, dass hohe, durch Muskeln erzeugte, Kräfte oder Drehmomente ACL Verletzungen verursachen, jedoch nie das Gegenteil. Ein Mangel an ausreichendem Schutz durch Co-Kontraktion sowohl der Knie- als auch Hüftmuskulatur wird selten als Ursache der ACL-Verletzung angesehen, obwohl diese mehr plausibel wäre.
In thisperspectivearticle, wepropose a new non-contactmechanismofinjurythatisinherently different fromextantmechanismsandprovides a morecompletepictureoftheeventsleadingtoinjury. • Weproposethat ACL injuryoccursbecauseoftheconcurrenceofspecificneuromuscularevents, externalloads due togroundcontact/impact, andcertainsubject-specificanatomicaldisadvantages. • The theorizedmechanismisthat non-contact ACL injuryoccurswhenthefollowingfactorsconverge: • delayedorslowco-activationofquadricepsandhamstringsmuscles, • a dynamicgroundreactionforceappliedwhilethekneeisnearfullextension • a shallow medial tibialplateauand a steepposteriortibialslope • a stifflanding due toincompatible hip andkneeflexionvelocities.
2.1. Delayedorslowco-activationofquadricepsandhamstringmuscles Itiswellknownthatco-contractionofthequadricepsandhamstringmusclesprovidesactiveprotectionforthekneeandits passive restraints…. Wesuggestthat a lossofactivetibiofemoralstability, resulting in increasedreliance on passive structures, is a necessary (but not sufficient) conditionfor ACL injury. Wesuggestthat all participants, male orfemale, aresusceptibletothisdelay. Wir weisen darauf hin, dass alle Teilnehmer, männlich oder weiblich, anfällig für diese Verzögerung sind.
2.2. Applicationof an impulsive groundreactionforcewhilethekneeisnearfullextension Sagitale Ebene JCF…jointcompressiveforce QPF…quadricepspatellar tendonforce HF…hamstringforce GRF…groundreactionforce (couldexceed 4000N) = + Roter Pfeil ist leicht verwirrend. Exaktere Erklärung ist auf der nächsten Seite dargestellt. Annahmen: Keine Beugung im Kniegelenk Ohne Reibung muss die JCF normal zur Kontaktfläche wirken GRF wirkt senkrecht, d.h. es wirkt keine Reibungskraft am Boden Keine Muskelkraft wirkt, da die Muskeln mit Verzögerung aktiviert werden. Ebenfalls verwirrend, dass die Muskelkräfte eingezeichnet sind.
2.2. Applicationof an impulsive groundreactionforcewhilethekneeisnearfullextension Posteriorfemurtranslationforce (Zerlegung der GRF in PFTF und JCF) Die ReibungskraftimKniegelenkzwischen tibia und femur wird in dieserArbeitnichtberücksichtigt. „Anteriortibialtranslationforce“ bewirkt eine Bewegung der Tibia Richtung anterio, bzw. eine Bewegung des Femur in Richtung posterior Je größer die „posteriortibialslope“ desto größer die anteriortibialtranslationforce Vergleiche dazu Hangabwärtstreibende Kraft beim Skifahren Anteriortibialtranslationforce (Zerlegung der GRF)
2.2. Applicationof an impulsive groundreactionforcewhilethekneeisnearfullextension In the literature, there are numerous assertions that the ACL is the primary restraint against anterior tibial translation at low flexion angles. If this is true, during landing near full extension, with a delay in co-contraction of quadriceps and hamstring muscles, there is see- mingly no protective mechanism to stop anterior tibial translation other than the ACL. However, this begs the question, ‘‘If delayed co- activation of quadriceps and hamstring muscles (for instance, due to fatigue) and a dynamic ground reaction force are all that is required for injury, why are higher ACL injury rates not observed?’’ The answer to the above question is that, according to literature, there are many other mechanisms by which the ACL is protected from injury, even if a deficiency in muscular protection occurs. Several of these protective mechanisms will be discussed in later sections.
2.3.1. Posterior slope of the tibial plateau and its orientation relative to the femur BeigebeugtemKniegelenk und gleicherÜberlegungergibtsich: The JCF, which is again perpendicular the plateau, will be directed posteriorly. This creates a posteriorly directed shear force shown by the red arrow which will resist anterior tibial translation. D.hbeigebeugtemKnieerzeugt die Bodenreaktionskraft GRF eine Kraft, welche die Tibia nachhintendrückt.
2.3.1. Posterior slope of the tibial plateau and its orientation relative to the femur
2.3 Posterior slope of the tibial plateau and its orientation relative to the femur Wilk et al. (1996) reported the generation of posteriorly directed shear forces in flexion angles ranging from 12° to 104° in squatting and 18° to 104° in leg press. The large joint compressive forces reported (6139 N in squats and 5762 N in leg press) must be directed posteriorly, as shown in Fig. 2b, to create an overall posteriorly directed shear force in the presence of anteriorly directed patellar tendon (quadriceps) forces. Lutz et al. (1993) report similar findings, showing posteriorly directed shear forces acting on the tibia in closed kinetic chain exercises at flexion angles of 30–90° . ScherkraftwirktnachhintenbeidiesenBeugewinkelbereichen. Biomechanically, it could be argued that this posteriorly directed component of the JCF plays an equal, if not greater ACL protective role than the posteriorly directed component of the hamstrings force. Subjects with mild tibial slope will benefit from this protection after very small amounts of knee flexion. On the contrary, subjects with steep tibial slopes will experience this added benefit only after moderate knee flexion.
2.3.2 Shallow medial tibial plateau depth It has also recently been shown that the depth of the medial tibial concavity may be a more critical risk factor in anterior. Those subjects with shallow or flat medial tibial plateaus, such as the one shown in Fig. 3a are at 3 times greater risk of injuring their ACLs for a 1 mm decrease in the depth of concavity. Deeper plateaus, such as the one in Fig. 3b, provide more stable seating of the medial femoral condyle on the tibial plateau.
2.4. A stiff landing due to incompatible hip and knee flexion velocities in the sagittal plane Fall1: WennUnter- wieOberschenkel wieabgebildet (grauePfeile) gedrehtwerden, bewegtsich das Knieeinfachnachvorne und eskommtzukeiner Translation zwischen Tibia und Femur Fall 2: WennUnter- und Oberschenkelwieabgebildet (grau, rote Pfeile) gedrehtwerden, kanndadurcheinerückwärtsgerichtete Translation des Femurs gegenüber der Tibia erfolgen. EineDrehung des OS gegen den UhrzeigersinnkanndurcheinezustarkeMuskelaktivierung der Hüftstreckererfolgen. Beispiel: Landen in RücklagebeimSkifahrenimsteilenGelände
An in-vitro study of joint geometry and loading effects on anterior cruciate ligament strain and knee kinematics Breighner, Ryan 2012 http://repositories.tdl.org/tdl-ir/handle/2346/45231 To better understand the influence of tibial geometry on ACL strain and injury, several studies of various knee-loading conditions were conducted on cadaver knees. The knees were first imaged using MRI, and measurements of their respective tibial geometries were taken. Subsequently, the knees were installed in the simulator and muscle forces were applied. In one of these studies, hip extensor-generated joint compressive forces were also applied, followed by an impulsive ground reaction force. The results of these studies indicate that tibial slope and medial tibial depth are significant predictors of ACL strain and that prelanding joint compression is protective of the ACL under dynamic loading. Additionally, it was shown that MCL strain increases more appreciably as a result of valgus loading as compared to the ACL. This information, coupled with the material properties of the two ligaments suggest that isolated ACL injury cannot result from purely valgus loadings. In vitro: unter künstlichen Bedingungen im Labor beobachtet oder durchgeführt In vivo: im lebenden Objekt, am lebenden Organismus beobachtet oder durchgeführt
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms Jason W. Levine,* MD, Ata M. Kiapour,* MS, Carmen E. Quatman, Nov. 2012 Background: The functional disability and high costs of treating anterior cruciate ligament (ACL) injuries have generated a great deal of interest in understanding the mechanism of noncontact ACL injuries. Secondary bone bruises have been reported in over 80% of partial and complete ACL ruptures. Purpose: The objectives of this study were (1) to quantify ACL strain under a range of physiologically relevant loading conditions and (2) to evaluate soft tissue and bony injury patterns associated with applied loading conditions thought to be responsible for many noncontact ACL injuries. Study Design: Controlled laboratory study. Methods: Seventeen cadaveric legs (age, 45 6 7 years; 9 female and 8 male) were tested utilizing a custom-designed drop stand to simulate landing. Specimens were randomly assigned between 2 loading groups that evaluated ACL strain under either knee abduction or internal tibial rotation moments. In each group, combinations of anterior tibial shear force, and knee abduction and internal tibial rotation moments under axial impact loading were applied sequentially until failure. Specimens were tested at 25° of flexion under simulated 1200 N quadriceps and 800 N hamstring loads. A differential variable reluctance transducer was used tocalculate ACL strain across the anteromedial bundle. A general linear model was used to compare peak ACL strain at failure. Correlations between simulated knee injury patterns and loading conditions were evaluated by the chi²test for independence.
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms Jason W. Levine,* MD, Ata M. Kiapour,* MS, Carmen E. Quatman, Nov. 2012 Results: Anterior cruciate ligament failure was generated in 15 of 17 specimens (88%). A clinically relevant distribution of failure patterns was observed including medial collateral ligament tears and damage to the menisci, cartilage, and subchondral bone. Only abduction significantly contributed to calculated peak ACL strain at failure (P = .002). While ACL disruption patterns were independent of the loading mechanism, tibial plateau injury patterns (locations) were significantly (P = .002) dependent on the applied loading conditions. Damage to the articular cartilage along with depression of the midlateraltibial plateau was primarily associated with knee abduction moments, while cartilage damage with depression of the posterolateraltibial plateau was primarily associated with internal tibial rotation moments. Conclusion: The current findings demonstrate the relationship between the location of the tibial plateau injury and ACL injury mechanisms. The resultant injury locations were similar to the clinically observed bone bruises across the tibial plateau during a noncontact ACL injury. These findings indicate that abduction combined with other modes of loading (multiplanar loading) may act to produce ACL injuries.
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms Testing Apparatus A custom-designed testing apparatus was used to simulate landing from a jump under a wide range of loading conditions (Figure 1). Each specimen was rigidly fixed at the proximal femur to a 6-axis load cell, while the tibia was orientated vertically with the foot positioned superiorly. All specimens were tested at 25° of flexion. The load cell was suspended such that the orientation of the femur could be rotated about all 3 axes to align the tibia with the vertical loading axis. A mass pulley system was used to apply 1200 N to the quadriceps tendons and 800 N to the hamstring tendons, while maintaining the physiological line of action of each tendon. Analog datawerecollectedat 4 kHz. Twoarraysof 3 infrared light-emittingdiodemarkerswererigidlyattachedtothefemurandtibiatocapturekneekinematics using an Optotrak 3020 (Northern Digital, Waterloo, Ontario, Canada) 3-dimensional motioncapturesystemat 400 Hz. The ACL strain was calculated based on measurements from a differential variable reluctance transducer (DVRT) with a linear range of 3 mm that was arthroscopically placed on the anteromedial (AM) bundle of the ACL.
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms Testing Apparatus The ACL strain was calculated based on measurements from a differential variable reluctance transducer (DVRT) with a linear range of 3 mm that was arthroscopically placed on the anteromedial (AM) bundle of the ACL. Sehr professionelle Lösung zur Erfassung der ACL-Kräfte bei einem Kniekadaver http://www.youtube.com/watch?v=athYrUMk2Ik&list=PLu0YtbFBcm4bmpV0gKp4E-IQyKI-Mhjsx&index=1 Weitere ACL Kadaver Untersuchung beim Laufen http://p3.smpp.northwestern.edu/Project/ACL.htm Anatomievideo Knie http://www.youtube.com/watch?v=_q-Jxj5sT0g
Clinically Relevant Injury Patterns After an Anterior Cruciate Ligament Injury Provide Insight Into Injury Mechanisms Weitere ACL Kadaver Untersuchung beim Laufen http://p3.smpp.northwestern.edu/Project/ACL.htm