Download
1 / 99
1.01k likes | 1.35k Vues
Hormonal Regulation Of Plasma Calcium And Calcium Metabolism. Guo Xiaosun guoxiaosun@126.com Shandong University. 1. The significance of maintaining plasma calcium levels. I The normal value and source of plasma calcium; II The structure, functions and endocrinology of bone;

E N D
Hormonal Regulation Of Plasma Calcium And Calcium Metabolism Guo Xiaosun guoxiaosun@126.com Shandong University
1. The significance of maintaining plasma calcium levels. I The normal value and source of plasma calcium; II The structure, functions and endocrinology of bone; 2. The hormonal regulation of plasma calcium: I Parathyroid hormone: parathyroid glands; secretion of parathyroid hormone; actions of parathyroid hormone; parathyroid hormone related peptide. II Calcitriol: source and activation of vitamin D; vitamin D and calcitriol in blood;action of calcitriol. III other hormones. 3. Disorders of calcium metabolism and metabolic bone disease: I Disorders of hypocalcaemia: vitamin D deficiency; parathyroid hormone deficiency. II Diseases of bone: osteoporosis; osteomalacia and rickets; Paget’s disease. 4. Regulation of serum phosphate.
1.The significance of maintaining plasma calcium levels.
CALCIUM • 2% of body weight • 99% in bones • 1% in body fluids • Plasma (Extracellular fluid) • 2.25 – 2.75 mmol/l • Cell (Intracellular fluid) • 10-8 – 10-7 mol/l = 10-5 – 10-4mmol/l
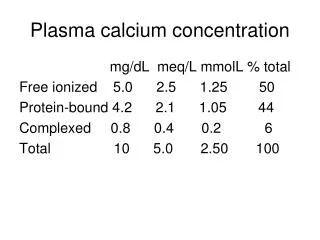
PLASMA CALCIUM diffusible 48% (50%) Ca2+ ionized 6% (10%) combined with anions (citrate, phosphate) – non-dissociated nondiffusible 46% (40%) combined with plasma proteins combination with proteins depends on pH0.2 mmol/l Ca2+ on each pH unit
Plasma Calcium Regulation • Free calcium is tightly regulated (5%) • Too low = neuronal hyper-excitability • Too high = neuronal depression • Control points for calcium • Absorption – Via intestines • Excretion – Via urine • Temporary storage – Via bones
Calcium Balance • Intake = output • Negative calcium balance: Output > intake • Neg Ca2+ balance leads to osteoporosis • Positive calcium balance: Intake > output • Occurs during growth • Calcium is essential, we can’t synthesize it
Calcium and the Cell • Translocation across the plasma membrane • Translocation across the ER and mitochondrion; Ca2+ATPase in ER and plasma membrane
ROLE OF CALCIUM excitability of cell membranes neuromuscular transmission and muscle contraction releasing of transmitters from synapses “second messenger” stimulates secretory activity of exocrine glands and releasing of hormones contractility of myocard blood coagulation
Changes in Ca2+ plasma level Hypocalcemia Muscle tetany carpopedal spasm Na+ inflow ↑→myocardium excitability and conductibility ↑; Ca2+ inflow ↓→plateau phase of action potential↑ Increased cell membrane permeability Impaired blood clotting Hypercalcemia Depression of nervous system, reflex activity, Increased heart contractility Formation of calcium phosphate crystalls(Kidney stones, and ectopic calcification)
Bones – reservoir of calcium • 99% of skeletal calcium forms stable bone (not exchangeable with the Ca in extracellular fluid) • 1% is in the form of releasable pool of Ca • Balance of deposition and resorption • Osteoblasts – bone-forming cells responsible for bone deposition • Secrete type I collagen • Differentiate into osteosytes • Osteoclasts – “bone-eating” cells that resorb the previously formed bone
Osteoblast and Osteoclast Function • Osteoblasts • Bone formation • Synthesis of matrix proteins • Type I collagen • Osteocalcin • Others • Mineralization • Activation of osteoclasts via RANKL production • Osteoclasts • Bone resorption • Degradation of proteins by enzymes • Acidification • RANK is activated by RANKL, and this leads to cells differentiation to osteoclasts
Regulation of osteoblasts function • Stimulation • PTH (fast reaction - activation of calcium pump ? – pumping Ca to ECF) • 1,25 Dihydrocholecalciferol • IL-1 • T3, T4 • hGH, IGF-1 (insuline-like growth factor) • PGE2 (prostaglandine) • TNF (tumor necrosis factor) • Estrogens • Inhibition • Corticosteroids
Regulation of osteoclasts function • Stimulation • PTH (not directly – through stimulation of osteoblasts) • 1,25 Dihydrocholecalciferol (not directly – through stimulation of osteoblasts) • IL-6, IL-11 • Inhibition • Calcitonin (directly – receptors) • Estrogens (by inhibiting production of certain cytokines) • TGF-β (tranforming growth factor) • PGE2(prostaglandine)
2. The hormonal regulation of plasma calcium
Regulation of calcium metabolism • Parathyroid hormone • Calcitonin • Vitamin D
Parathyroid Hormone Structure • Synthesized in the 4 para-thyroid glands • PreProPTH Regulator of Ca2+ homeostasis • PTH t1/2 (half life) is 2-3 min • Liver (2/3rds) and kidney (1/3rd) are major sites of fragmentation
W.F.Ganong: Review of Medical Physiology 2003 20th Ed. #188 fig.21-10
Mechanism of Action of PTH PTH binds to a G protein-coupled receptor. Binding of PTH to its receptor activates 2 signaling pathways: - increased cyclic AMP - increased phospholipase C Activation of PKA appears to be sufficient to decrease bone mineralization Both PKA and PKC activity appear to be required for increased resorption of calcium by the kidneys
Actions of PTH: Bone PTH acts to increase degradation of bone (release of calcium). --Rapid action --Delayed action - causes osteoblasts to release cytokines, which stimulate osteoclast activity - stimulates bone stem cells to develop into osteoclasts -- net result: increased release of calcium from bone -- effects on bone are dependent upon presence of vitamin D
Actions of PTH: Kidney • PTH acts on the kidney →the reabsorption of calcium ↑ (excretion↓). • excretion of phosphate ↑ excretion of H+↓(more acidic environment favors demineralization of bone) • ALSO, Stimulates transcription of 1-alpha hydroxylase for Vitamin D activation in kidney→the active metabolite ofvitamin D3↑(required for calcium absorption from the small intestine, bone demineralization). • NET RESULT: increased plasma calcium levels
Regulation of PTH Secretion PTH is released in response to changes in plasma calcium levels (negative feedback). PTH cells contain a receptor for calcium, coupled to a G protein. calcium ↑→ Gq →PLC→IP3 →calciuminflow↑,ER calciumrelease↑→ PTH ↓ Also, vitamin D↑,Mg2+↑, P↓,somatostatin→PTH↓
Effects of Active Form of Vit D3 Promotes intestinal absorption of calcium promotes bone mobilization (stimulate osteoclasts’ precursor mature and turnover →Ca2+↑Pi ↑)mainly promotes bone deposition (stimulate osteoblasts → osteocalcin↑other protein↑→deposition ↑ calcification ↑) Has slight effect to increase calcium re-absorption in kidneys Works with PTH to cause calcium absorption from bone PTH↓
Proposed Mechanism of Action of 1,25-DihydroxyD3 in Intestine
Regulation of Vitamin D Metabolism PTH→1-hydroxylase activity↑→ production of active form↑ PTH→ 24-hydroxylase transcription↓→1,24,25(OH)3D 3↓ phosphate ↓→ 1-hydroxylase activity↑ Ca↓→PTH→………… 1,25 (OH)2D 3↑→ 1-hydroxylase activity ↓ 1,25 (OH)2D 3↑→ 24-hydroxylase transcription↑→ 1,24,25(OH)3D 3↑ Growth hormone, prolactin, estrogen, calcitonin→ 1,25 (OH)2D 3↑ cortisol → 1,25 (OH)2D 3 ↓
Changes in vitamine D plasma level Hypovitaminosis • RICKETS (rachitis)– children • OSTEOMALACIA - adults • Attention! – Osteoporosis is decrease of bone mass (matrix and minerals) Hypervitaminosis • Tissue and organs calcification • Lost of body weight • Kidney function failure
Calcitonin Product of parafollicular C cells of the thyroid 32 aa
Actions of Calcitonin • The target cell for calcitonin is the osteoclast. --Calcitonin acts via increased cAMP concentrations to inhibit osteoclast motility and cell shape and inactivates them. (15min ↓70%,mainly in children but not in adult) --The major effect of calcitonin administration is a rapid fall in Ca2+ caused by inhibition of bone resorption. • osteoblastic activity ↑→Ca P deposition ↑(1h) • Ca, P , Mg, Na and Cl resorption in kidney tubules ↓(weak)
Comparison of Calcitonin Effects with PTH Effects (1) PTH ---- slowly, need several hrs. CT ----- rapidly, less than 1 hr. (2) PTH ---- long-term regulation CT ----- short-term regulation PS Wang/2004.05
What is the Role of Calcitonin in Humans? Removal of the thyroid gland has no effect on plasma Ca levels! Excessive calcitonin release does not affect bone metabolism! Other mechanisms are more important in regulating calcium metabolism (i.e., PTH and vitamin D).
Calcitonin Role of calcitonin in normal Ca2+ control is not understood—may be more important in control of bone remodeling. Used clinically in treatment of hypercalcelmia and in certain bone diseases in which sustained reduction of osteoclastic resorption is therapeutically advantageous. May be more important in regulating bone remodeling than in Ca2+ homeostasis.
Regulation of Calcitonin Release Food (high calcium ) gastrin, CCK, glucagon, secretin increased calcitonin decreased bone resorption Calcitonin release is stimulated by increased circulating plasma calcium levels. Calcitonin release is also caused by the gastrointestinal hormones gastrin and cholecystokinin (CCK), whose levels increase during digestion of food.
Factors affecting bone turnover • Other hormones • Glucocorticoids • gut - decrease absorption • bone - increased re-absorption/decreased formation • Kidney-excretion of both calcium and phosphate ↑ • Thyroxine • stimulates formation/resorption • net resorption • Kidney-excretion of calcium↑ • Growth hormone • Stimulate bone formation • renal calcium excretion ↑ • gastrointestinal absorption of calcium ↑ • Oestrogen • gut - increased absorption • bone - decreased re-absorption
Estrogens and Androgens: both stimulate bone formation during childhood and puberty. Estrogen inhibits PTH-stimulated bone resorption. Estrogen increases calcitonin levels Osteoblasts have estrogen receptors, respond to estrogen with bone growth. Postmenopausal women (low estrogen) have an increased incidence of osteoporosis and bone fractures.
W.F.Ganong:Review of Medical Physiology 2003 20th Ed. fig.21-6 #1441
Factors affecting bone turnover • Local factors • I-LGF 1 (somatomedin C) • increased osteoblast prolifn • TGF • increased osteoblast activity • IL-1/OAF • increased osteoclast activity (myeloma) • PG’s • increased bone turnover (#’s/inflammn) • BMP • bone formation
Factors affecting bone turnover • Other factors • Local stresses • Electrical stimuli • Environmental • temp • oxygen levels • acid/base balance