Tumour immunology
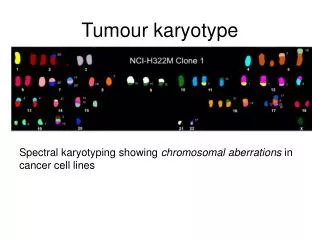
Tumour immunology. J. Ochotná. Tumor antigens. Antigens specific for tumors (TSA) complexes of MHC gp I with abnormal fragments of cellular proteins - chemically induced tumors - leukemia with chromosomal translocation


Tumour immunology
E N D
Presentation Transcript
Tumour immunology J. Ochotná
Tumor antigens • Antigens specific for tumors (TSA) • complexes of MHCgp I with abnormal fragments of cellular proteins- chemically induced tumors - leukemia with chromosomal translocation • complexes of MHCgp with fragments of proteins of oncogenic viruses- tumors caused by viruses (EBV, SV40, polyomavirus) • abnormal forms of glycoproteins- sialylation of surface proteins of tumor cells • idiotypes of myeloma and lymphoma- clonotyping TCR and BCR
b) Antigensassociatedwithtumors (TAA) • presentalso on normalcells • differences in quantity, timeandlocalexpression • auxiliarydiagnosticmarkers onkofetalantigens • on normalembryoniccellsandsome tumor cells • -fetoprotein (AFP) - hepatom • carcinoembryonic antigen (CEA) - coloncancer melanomaantigens • MAGE-1, Melan-A
antigen HER2/neu • receptor forepithelialgrowthfactor • mammarycarcinoma EPCAM • epithelialadhesionmolecule • metastases differentiationantigensofleukemiccells • present on normalcellsofleukocyteslinage • CALLA -acutelymphoblasticleukemia (CD10 pre-B cells)
Anti-tumor immune mechanisms Immunecontrol • tumor cellsnormallyarise in tissues and are eliminated by Tlymphocytes Defensiveimmune response • tumor cells are weaklyimmunogenic • occurswhen tumor antigens are presented to T lymphocytesby dendriticcellsactivated in theinflammatoryenvironment
if tumor cells are detected, in defense maybeinvolvednon-specificmechanisms(neutrophilicgranulocytes, macrophages, NK cells, complement) andantigen-specificmechanisms(TH1 and TC, antibodies)
DC are necessaryforactivationof antigen specificmechanisms • cancer-associatedantigens are processed by DC andrecognized by T lymphocytes in complexwith HLA I. and II. classwithprovidingcostimulussignals • predominance ofTH1(IFN g, TNFa) • specific cell-mediatedcytotoxicreactivity –TC • activationof TH2 → support B lymphocytes→ tumor specificantibodies (involved in the ADCC) • tumor cells are destroyed by cytotoxicNK cells (ADCC) • interferons - antiproliferative, cytotoxiceffect on tumor cells - INFγ - DC maturation
Regulatory T cellsprevents removal of cancer cells and thus contribute to the development of the tumor.
Mechanisms of tumor resistance to the immune system - • high variability of tumor cells • low expression of tumor antigens • sialylation • tumor cells signals do not provide costimulus → T lymphocyte anergy • some anticancer substances have a stimulating effect • production of factors inactivating T lymphocytes • expression of FasL → T lymphocyte apoptosis • inhibition of the function or durability dendritic cells (NO, IL-10, TGF-b)
Transplantation = transfer of tissue or organ ●autologous - donor = recipient ● syngeneic - genetically identical donor and recipient (identical twins) ● allogeneic - genetically nonidentical donor of the same species ● xenogenic - the donor of another species ● implant - artificial tissue compensation
Allotransplantation ●differences in donor-recipient MHC gpandsecondaryhistocompatibilityAg ●alloreactivityof T lymphocytes - the risk ofrejectionandgraft-versus-host disease ●directdetectionofalloantigens – recipient T lymphocytesrecognizethedifferent MHC gpand non-MHC molecules on donor cells ●indirectrecognitionofalloantigens - APC absorbdifferent MHC gpfrom donor cellsandpresentthefragments to T lymphocytes
Testing before transplantation ●ABOcompatibility -risk of hyperacute or accelerated rejection (= formation of Ab against A or B Ag on graft vascular endothelium) ●HLA typing (determining of MHC gp alelic forms) phenotyping and genotyping by PCR ●Cross-match - lymphocytotoxic test – detection of preformed Ab (after blood transfusions, transplantation, repeated childbirth) ●Mixed lymphocyte reaction - testing of T lymphocytesalloreactivity, monitor for reactivity of lymphocytes to allogeneic HLA
HLA typing = determmination of HLA antigens on the surface of lymphocytesCarry out during the testing before transplantation and in determination of paternity • 1) Serotyping • Microlymfocytotoxic test • Allospecificserums (obtainedfrom multiple natal to 6 weeksafterbirth, obtained by vaccinationofvolunteers, orcommerciallypreparedsetsoftypingserums (monoclonalantibodies)) • Principle - theincubationoflymphocyteswithtypingserums in the presence ofrabbitcomplement, thenisaddedthevitaldyewhichstaineddeadcells - cellscarryingspecific HLA are killed by cytotoxic Ab againsttheAg, thepercentageofdeadcellsis a measureofserum toxicity (forcesandantileukocyteantibody titre) • Positive reactionisconsidered more than 10% deadcells(serologicaltypingcanbedonealso by flowcytometry
2) Molecular genetic methods 2a) PCR-SSP = Polymerase chain reaction with sequential specific primers • Extracted DNA is used as a substrate in a set of PCR reactions • Each PCR reaction contains primers pair specific for a certain allele (or group of alleles) • Positive and negative reactions are evaluated by electrophoresis, each combination of alleles has a specific electrophoretic painting
2b) PCR-SSO • PCR reaction with sequence-specific oligonucleotides Multiplication of hypervariable sections of genes coding HLA • Hybridization with enzyme or radiolabeled DNA probes specific for individual alleles 2c) PCR-SBT • Sequencing based typing • The most accurate method of HLA typing • We get the exact sequence of nucleotides, which compares with a database of known sequences of HLA alleles
Cross-match testing ● determination of preformed antibodies ● recipient serum + donor lymphocytes + rabbit complement → if cytotoxic Ab against donor HLA Ag are present in recipient serum (called alloantibodies = Ab activating complement) → lysis of donor lymphocytes. Visualization of dye penetration into lysis cells. ●positive test = the presence of preformed Ab → risk of hyperacute rejection! → contraindication to transplantation
Mixedlymphocytereaction (MRL) ●determinationof T lymphocytesalloreactivity ●mixed donor and recipient lymphocytes → T lymphocytesafterrecognitionofallogeneic MHC gpactivateandproliferate One-way MRL ●determinationof recipient T lymphocytesreactivityagainst donor cells ● donor cellstreatedwithchemotherapyorirradiated lose theabilityofproliferation
Immunologically privileged sites and tissues • Transplantationofsometissues don´t lead to theinductionofallogeneicreactivity • Evolutionarilysignificant, protectionofvitalorgans (brain, eye, gonads) • Factorsprotectingimmunologicallyprivilegedstructures • isolationfromtheimmunesystem (minimalcontentoflecocytes) • preference of TH2 reactoin, supressionof TH1 reaction • FasLexpression • productionofTGFb
Hyperacute rejection ● minutes to hours after transplantation ●humoral mediated immune response mechanism: ● if in recipients blood are present preformed or natural Ab (IgM anti-carbohydrate Ag) before transplantation→ Ab + Ag of graft (MHC gp or endothelial Ag) → graft damage by activated complement (lysis of cells) ● the graft endothelium: activation of coagulation factors and platelets, formation thrombi, accumulation of neutrophil granulocytes prevention: ● negative cross match before transplantation, ABO compatibility
Acceleratedrejection ● 3 to 5 daysaftertransplantation ●caused by antibodiesthat don´t activatecomplement ●cytotoxicandinflammatoryresponsestriggered by bindingofantibodies to Fc-receptors on phagocytesand NK cells prevention: ● negative crossmatchbeforetransplantation, ABOcompatibility
Acute rejection ● days to weeks after the transplantation or after a lack of immunosuppressive treatment ●cell-mediated immune response mechanism: ● reaction of recipient TH1 and TC cells against Ag of graft tissue ● infiltration by lymphocytes, mononuclears, granulocytes around smallvessels → destruction of tissue transplant
Chronic rejection ● from 2 months after transplantation ● the most common cause of graft failure mechanism is not fully understood: ● non-immunological factors (tissue ischemia) and TH2 responses with production alloantibodies, pathogenetic role of cytokines and growth factors (TGF β) ● fibrosis of the internal blood vessels of the transplanted tissue, endothelial damage →impaired perfusion of graft → gradual loss of its function dominating findings: vascular damage
Rejection Factors: ●The genetic difference between donor and recipient, especially in the genes coding for MHC gp (HLA) ●Type of tissue / organ - the strongest reactions against vascularized tissues containing many APC (skin) ●The activity of the recipientimmune system - the immunodeficiency recipient has a smaller rejection reaction; immunosuppressive therapy after transplantation – suppression of rejection ●Status of transplanted organ - the length of ischemia, the method of preservation, traumatization of organ at collection
Bone MarrowTransplantation ●Removalofhematopoietic stem cells●Myeloablation●Transplantation●Engraftment●Rejection●Graft-versus-host reaction
Graft-versus-host (GvH) disease ● after bone marrow transplantation ● GvH also after blood transfusion to immunodeficiency recipients ● T-lymphocytes in the graft bone marrow recognize recipient tissue Ag as foreign (alooreactivity)
Acute GvH disease ● days to weeks after the transplantation of stem cells ● damage of liver, skin and intestinal mucosa ● prevention: appropriate donor selection, the removal of T lymphocytes from the graft and effective immunosuppression
Chonic GvH disease ● months to years after transplantation ● infiltration of tissues and organs by TH2 lymphocytes, production of alloantibodies and cytokines → fibrosis ● process like autoimmune disease: vasculitis, scleroderma, sicca-syndrome ● chronic inflammation of blood vessels, skin, internal organs and glands, which leads to fibrosis, blood circulation disorders and loss of function
Graft versus leukemia effect (GvL) ● donor T lymphocytes react against residual leukemick cells of recipient (setpoint response) ● mechanism is consistent with acute GvH ● associated with a certain degree of GvH (adverse reactions)
Immunologic relationship between mother and allogenic fetus ●fetal cells have on the surface alloantigens inherited from his father ●pregnancy = "semiallogenic transplantation“ Tolerance of fetus by mother allow the following mechanisms: ●the relative isolation of the fetus from maternal immune system (no mixing of blood circulation) ●trophoblast - immune barrier witch protects against mother alloreactive T lymphocytes - don´t express classical MHC gp, expresses non-classical HLA-E and HLA-G ● transfer of small doses of fetal antigens in maternal circulation causes tolerance ... suppressin of TH1 and preference of TH2 immune mechanisms in pregnancy
Rh incompatibility • Complications in pregnancy: production of anti-RhD antibodies by RhD- mother carrying an RhD+ fetus (hemolytic disease of newborns) • Fetal erythrocytes penetrate into the maternal bloodstream during pregnancy - a small amount, don´t immunize • During childbirth or abortion (after 8 weeks of gestation) fetal erythrocytes can penetrate into the bloodstream of mother → immunization, formation of anti-RhD antibodies • After childbirth, investigate Rh factor of born child, if is child Rh+, mother gets up to 72 hours after birth injection of anti-Rh antibodies (administered after abortion too)
Anti-Rh(D) injection, thisantibodiesbind to RhDAg on baby´s redbloodcells, thisAgthancan´t bind to BCR andcan´t activate B lymphocytes, thisimmunecomlexesalsoactivelyinhibit B lymphocytes • Duringnextchildbirths, if fetus isRh+ andmotherproduceanti-Rhantibodies, thisAbbdestroyredbloodcellsof fetus, whichcanlead to fetaldeath, or in severe postpartumanemia(anemianeonatorum)andneonataljaundice (icterus gravis neonatorum) • ForeachpregnantwomanduringthefirsttrimesterinvestigateblodRhfactorandthe presence ofantibodies, in Rh- womenperformed a test forantibodiesalso in II. and III. trimester
Classification by Coombs and Gell Immunopathological reactions: immune response, which caused damage to the body (secondary consequence of defense responses against pathogens, inappropriate responses to harmless antigens, autoimmunity) IV types of immunopathological reactions: Type I reaction - response based on IgE antibodies Type II reaction - response based on antibodies, IgG and IgM Type III reaction- response based on the formation of immune complexes Type IV reaction - cell-mediated response
Immunopathological reactions based on antibodies IgG and IgM (reaction type II) Cytotoxic antibodies IgG and IgM: ● complement activation ● binding to Fc receptors on phagocytes and NK cells (ADCC)
Examples of immunopathological reaction Type II • Transfusionreactionsafteradministrationofincompatibileblood: bindingofantibodies to antigens on erythrocytes → activationoftheclassicalpathwayofcomplement → cell lysis • Hemolyticdiseaseofnewborns:caused by antibodiesagainstRhD antigen
Autoimmune diseases: ● organ-specific cytotoxic antibodies (antibodies against erythrocytes, neutrophils, thrombocytes, glomerular basement membrane ...) ● blocking or stimulating antibodies Graves - Basedow's disease - stimulating antibodies against the receptor for TSH Myasthenia gravis - blocking of acetylcholin receptor→ blocking of neuromuscular transmission Pernicious anemia - blocking the absorption of vitamin B12 Antiphospholipid syndrome - antibodies against fosfolipids Fertility disorder - antibodies against sperms or oocytes
Immunopathological reactions based on immune complexes formation (reaction type III) ●caused by IgG antibodies → bind to antigen → creation of immune complexes ● immunocomplexes - bind to Fc receptors on phagocytes - activate complement ● immune complexes, depending on the quantity and structure, are eliminated by phagocytes or stored in tissues ● pathological immunocomplexes response arises when is a large dose of antigen, or antigen in the body remains; arise 10-14 days after aplication of Ag and induced inflamation can get to chronic state ● immune complexes are deposited in the kidneys (glomerulonephritis), on the surface of endothelial cells (vasculitis) and in synovie joint (arthritis)
Serum sickness ● the therapeutic application of xenogeneic serum (antiserum to snake venom) ● creation of immune complexes and their storage in the vessel walls of different organs ● clinical manifestations: urticaria, arthralgia, myalgia Systemic lupus erythematosus ● antibodies against nuclear antigens, ANA, anti-dsDNA Farmer's lung ● IgG antibody against inhaled antigens (molds, hay) Post-streptococcal glomerulonephritis, cryoglobulinemia, revmatoid arthritis, post-infectious arthritis
Tumor immunotherapy Therapy- surgical removal of tumor - chemotherapy or radiotherapy - immunotherapy Immunotherapy-induction of anti-tumor immunity, or the use of immune mechanisms to targeting drugs to the tumor site
Immunotherapy using antibodies Antibodies functions - opsonization - activation of complement - induction of ADCC - carriers of drugs or toxins
1) Monoclonal antibodies - against TAA - mouse and humanised antibodies - imunotoxins, radioimunotoxins - the possibility of damage surrounding tissues - HERCEPIN - Ab against HER2/neu, breast cancer - RITUXIMAB - Ab against CD20, lymphoma 2) Bispecific antibodies - bind a tumor antigen and the T lymphocyte or NK cell - Fc fragment of antibody binds to Fc receptors on phagocytes and NK cells 3) Elimination of tumor cells from the suspension of bone marrow cellsusing monoclonal antibodies for autologous transplantation
Immunotherapy using cell-mediated mechanisms 1) stimulation of inflammation at the tumor site 2) stimulation of LAK and TIL - isolation of T and NK cells, stimulation by cytokines, and return to the patient - LAK (lymphokine activated killers) - TIL (tumor infiltrating lymphocytes) 3)improving of tumor cells antigenpresenting function - genetic modification of tumor cells - expression of CD80, CD86 - production of IL-2, GM-CSF - modified cells are irradiated and returned to the patient
4) the dendritic cell immunotherapy- in vitro cultivation of monocytes in an appropriate cytokine environment (GM-CSF, IL-4) → transformation into dendritic cells- cultivation of dendritic cells with tumor antigens