Download
1 / 13
140 likes | 402 Vues
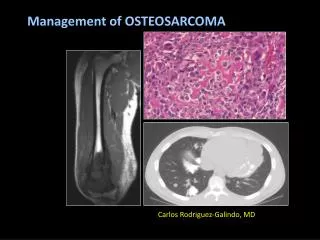
Non-metastatic Osteosarcoma: Response based augmentatation of therapy . P9754 A Children’s Oncology Group Study Schwartz CL, Wexler LH, Devidas M, Teot LA, Goorin A, Grier H, Gebhard M, Steinherz L, Sato J, Healey J, Lipshultz S, Miser J, Womer R, Meyers P, Bernstein M. P9754 BACKGROUND.

E N D
Non-metastatic Osteosarcoma: Response based augmentatation of therapy P9754 A Children’s Oncology Group Study Schwartz CL, Wexler LH, Devidas M, Teot LA, Goorin A, Grier H, Gebhard M, Steinherz L, Sato J, Healey J, Lipshultz S, Miser J, Womer R, Meyers P, Bernstein M
P9754 BACKGROUND • Percent necrosis (% NEC) is predictive of EFS • Dose Intensity is associated with outcome • Acute & long term cardiac toxicity significant • Understanding biology will allow prognosis
P9754:OBJECTIVES Although chemotherapy has improved outcome for OS, patients continue to experience recurrence and death. P9754 was designed to: • Evaluate the safety of augmenting chemotherapy with doxorubicin (600mg/m2 cumulative dose) or ifosfamide (14 g/m2/cycle). • Determine if dexrzoxane (DXR) cardioprotection during pre-operative induction chemotherapy affects histologic response. • Assess feasiblity of collecting tumor tissue for biologic investigation.
P9754: Sequential Pilot Studies to Augment Therapy • #1: Doxo intensification to 600mg/m2 with dexrazoxane • #2: Doxo intensification to 600mg/m2 with dexrazoxane and ifosfamide • #3: Ifosfamide/Etoposide intensification
CDDP: 120 mg/m2/cycle X4 MTX = 12 g/m2 X 12, Doxo 75 mg/m2 x 6 Therapy: P9754 Induction 10 weeks Surgery Post-op Chemotx GR Continue 3 drugs For 22 weeks Pilot 1 MTX, CDDP, Doxo Doxo Intensification 3 drugs with Doxo to 600 mg/m2 cum. SR Pilot 2 MTX, CDDP, Doxo Ifos (9g/m2) 4 drugs with Doxo to 600 mg/m2 cm. Continue 4 drugs for 22 weeks GR Pilot 3 MTX, CDDP, Doxo, Ifos Ifos/Etoposide Intensification SR 4 drugs with VP16/Ifos (14g/m2 /cycle)
Results: Sequential Pilots • Original projection: 60 patients/pilot, 90 SR • 253 enrolled, 242 eligible, 221 evaluate response • Surgical delay not evaluable Additional accrual to pilot 1 (DOXO @600 mg/m2) Pilot 1: 112 Pilot 2: 54 Pilot 3: 55 Pilot 1 9/1999 – 6/2000 Pilot 3 6/00- 1/00 Pilot 2 11/00 - 5/01 Pilot 1 5/01 – 10/01
Results: Toxicity At 30 months: mean FS 33.8 vs. 34.6 for 450 vs. 600 doxo treatment arms (based on very limited numbers entered on LE RDE form)
Response to Preoperative Chemotherapy: Percent Necrosis Historic Control (POG8651): 30% had > 98% Necrosis * Of those evaluable for response No adverse effect on % Necrosis with dexrazoxane
Event Free Survival for Good & Standard Response EFS at 4 yrs GR: 79.1 + 6.2% SR: 55.2 + 5.3% Pilot 1: EFS @ 4 yrs GR: 73.8 + 10.9% SR: 51.8 + 8.2% Pilot 2: EFS @ 4 yrs GR: 76.2 + 9.3% SR: 57.1 + 9.1% Pilot 3: EFS @ 4 yrs GR: 88.9 + 8.2% SR: 60.7 + 8.5%
EFS by Pilot EFS at 4 yr Pilot 1: 55.0 + 6.5% 2: 65.9 +8.6% 3: 70.0 + 6.5%
P9754 Overall Survival by pilot OS at 4 yr Pilot 1: 69.7 + 5.9% 2: 78.9 + 7.0% 3: 76.3 + 6.0%
Biologic Specimens • POG 9851: Biology Trial • Specimens submitted on 213 of 253 enrolled on P9754
Conclusions • Dose intensification • Feasible with high cumulative dose doxorubicin OR etoposide/high dose ifosfamide • EFS Difference of SR vs. GR. remains statistically significant • EFS/OS is similar to prior studies (eg. INT 0133) • No statistically significant difference between pilots at this time. Randomized studies needed to determine benefit of IE augmentation • Cardioprotection by Dexrazoxane • ~ 2% acute cardiotoxicity WITH DEXRAZOXANE: including patients receiving DOXO up to 600 mg/m2 • % NEC not reduced by Dexrazoxane vs. historical controls. Further studies should address the role of DXR in reducing long term anthracycline induced cardiotoxicity • Biology • Tumor banking was feasible: 84% submission rate