Download
1 / 28
280 likes | 430 Vues
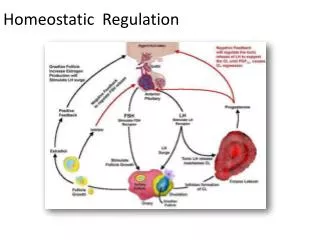
Exploring the homeostatic theory of SWB in a group of adolescents. Carrie Hayward & Mark Stokes Deakin University 2007. Background to research. Theory of SWB Homeostasis SWB held within a narrow positive range 70-80% Scale Maximum

E N D
Exploring the homeostatic theory of SWB in a group of adolescents Carrie Hayward & Mark Stokes Deakin University 2007
Background to research Theory of SWB Homeostasis • SWB held within a narrow positive range 70-80% Scale Maximum • Cummins has found SWB to be held at around 75% SM in normal adults populations internationally • The system is under the control of cognitive buffers.
Cognitive Buffers • Work to maintain SWB in the positive 70-80% range • Past research has explored the role of personality and control constructs Personality • Cummins, Gullone & Lau (2002) argue that personality mediates the relationship between external experiences and SWB. • Extroversion associated with positive affect, Neuroticism associated with negative affect • However, correlations vary significantly between studies, and the role of personality factors in the maintenance of SWB is questionable.
Cognitive Buffers Mastery • The perceived ability to bring about desired outcomes or responses • A global construct • Refers to control over internal self as well as actual control over environmental conditions. • Viewed to be a critical mediator between life stressors and health outcomes (Pearlin & Schooler, 1978).
Background research • The homeostatic system can be defeated by extreme negative experiential input • Commonly observed in individuals with traumatic brain injury (TBI). Q. Why do some individuals experience lower SWB following TBI?
Research Project • Research into the homeostatic theory of SWB in a TBI population was conducted, to compare with normative data. • However, existing research into the SWB of adolescents was limited and normative data was not available. • The aim of this study was therefore to obtain normative SWB data for adolescents.
Methodology Participants • 603 students (years 7 to 10) from two Melbourne schools. • Age range from 11-18 yrs (M = 14.3) • 480 Males & 123 Females Procedure • All senior level students were invited to participate. • Students who provided informed individual and parental consent were included in the sample. • Paper and pencil questionnaire was completed on allocated morning during home room.
Measures • PWI-SC – Personal Wellbeing Index – School Children 2nd Edition(Aust. Centre on QOL, Deakin University) How happy are you with your…. • Standard of living • Health • What you achieve in life • Personal relationships • Community connectedness (“doing things away from home”) • Safety • Future security * Participants rated each item on a 11-point Likert response scale ranging from (0) very sad to (10) very happy
Measures 2. Mastery Scale (Pearlin & Schooler, 1978) • Seven-item scale • Assesses the degree to which individuals perceive personal mastery over life outcomes e.g., "I can do just about anything I really set my mind to do". * Responses were given on a 11-point Likert response scale ranging from: (0) strongly disagree to (10) strongly agree.
Measures 3. The Big-Five Abridged Scale(BFAS; Langford, 2003) • Five-item scale of the Big Five framework of personality. Each item measuring: Openness: uncreative (0) vs. creative (10) Agreeableness: headstrong (0) vs. gentle (10) Conscientiousness: lazy (0) vs. hardworking (10) Extraversion: shy (0) vs. outgoing (10) Neuroticism: nervous (0) vs. at ease (10)
Measures Participants were also asked: • Have you ever experienced a knock to the head that resulted in a loss of conscious? • If yes: - Were you hospitalized? - How long were you hospitalised for? (no. of days/mths.) • 547 participants answered ‘no’ to both questions = the normative group. • 140 participants reported experiencing a knock to the head with no admission = the ambiguous group. • 56 participants experienced a knock to the head and were admitted to hospital = the head injured group. Length of stay ranged from ½ day to 30 days.
Aims and Hypotheses of Study 1 Aims • Determine the population mean of SWB in a group of normal adolescents. • Investigate the affect of personality and mastery on SWB in adolescents • Preliminary investigation into the association between previous head injury and SWB.
Hypotheses of Study 1 Hypotheses • Adolescent data would replicate adult data, with SWB population mean falling within 70-80% SM range. • Personality and Mastery would be associated with SWB. • Personality and Mastery would mediate the association between previous head injury and SWB.
Results – Hypothesis 1 Adolescent Population Means
Results – Hypothesis 1 Adolescent Population Means
Results – Hypothesis 1 T-Tests for Non-HI and HI mean SWB and Mastery responses
Results – Hypothesis 1 T-Tests for Non-HI and HI mean Personality responses *p = 0.01
Results – Hypothesis 2 Standard regression analysis testing the role of Mastery, Head Injury and Personality *p<.05; **p<.01; ***p<.001
Results – Hypothesis 2 Sequential regression analysis testing the role of Mastery and sig. Personality constructs *p<.05, **p<.01 ***p<.001
SWB SWB HI HI Mastery Personality Results – Hypothesis 3 Do Personality and Mastery mediate the effect of Head Injury on SWB? • Head Injury did not have a significant direct effect on SWB • However, mediation tests were carried out to determine if Head Injury had a significant indirect effect on SWB through the Personality and Mastery. Mediation Model 1 Mediation Model 2 c c b (Sb) a (Sa) b (Sb) a (Sa)
Results – Hypothesis 3 Mediation Model 1: Personality as mediator • One personality factor was extracted through the principal components method. • Personality factor explained 35.6% of variance: ²(10, N=603)=258.741, p<.001 • Sobel’s Test = To test whether a mediator carries the influence of an IV to a DV. Eqn. (1) * Sobel Test formula was drawn from MacKinnon & Dwyer (1994).
SWB HI Personality Results – Hypothesis 3 Mediation Model 1: Personality as mediator • Sobel’s Z was obtained to assess whether the indirect effect of Head Injury through Personality was significant. c b (Sb) a (Sa) ( ‘x’ ) = simple regression B weight Sobel’s Z = 1.206 (p=.228)
SWB HI Mastery Results – Hypothesis 3 Mediation Model 2: Mastery as mediator • Sobel’s Z was obtained to asses whether the indirect effect of Head Injury through Mastery was significant. c b (Sb) a (Sa) ( x ) = simple regression B weight Sobel’s Z = -1.512 (p=0.130)
Conclusion • Hypothesis 1 supported: SWB population mean for adolescents similar to adults, falling within positive range, 70-80% SM • Hypothesis 2 supported: • Mastery was a significant predictor of SWB. • Openness, conscientiousness, extraversion and neuroticism were significant predictors of SWB.
Conclusion • Hypothesis 3 not supported: • No significant direct effect of Head Injury on SWB. • Mastery and Personality did not mediate the effect of Head Injury on SWB.
Conclusion • The SWB of normative adolescents is similar to the SWB of normative adults (within the 70-80% normative range). • Results have provided support for the significant effect of Mastery and Personality on SWB. • Preliminary findings suggest that individuals who have sustained previous head-injury tend to be extraverted.
References • Cummins, R. A. (1995). On the trail of the gold standard for life satisfaction. Social Indicators Research, 35, 179-200. • Cummins, R. A., & Lau, A. L. D. (2004). The Motivation to Maintain Subjective Well-Being: A Homeostatic Model. In H. N. Switzky (Ed.), Personality and motivational systems in mental retardation: Vol. 28 (pp. 255-301). San Diego, CA: Elsevier Academic Press. • Cummins, R. A., Eckersley, R., Okerstrom, E., Hunter. B., & Davern, M. (2003). Australian Unity Wellbeing Index: Cumulative Psychometric Record Vol. 9. Melbourne: Australian Centre on Quality of Life, School of Psychology, Deakin University. • Cummins, R. A., & Nistico, H. (2002). Maintaining life satisfaction: The role of positive cognitive bias. Journal of Happiness Studies, 3, 37-69. • Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The satisfaction with life scale. Journal of Personality Assessment, 49, 71-75. • Gosling, S., Rentfrow, P. J., & Swann, W. B. Jr. (2003). A very brief measure of the Big-Five personality domains.Journal of Research in Personality, 37, 504-528. • Headey, B., & Wearing, A. (1989). Personality, life events, and subjective well-being: Toward a dynamic equilibrium model.Journal of Personality and Social Psychology, 57, 731-739. • Langford, P. H. (2003). A one-minute measure of the Big Five? Evaluating and abridging Shafer's (1999a) Big Five markers.Personality and Individual Differences, 35, 1127-1140. • MacKinnon, D. P., & Dwyer, J. H. (1993). Estimating mediated effects in prevention studies. Evaluation Review, 17, 144-158. • Paunonen, S. V., & Jackson, D. N. (1985c). The validity of formal and informal personality assessments. Journal of Research in Personality, 19, 331-342. • Pearlin, L. I., Menaghan, E. G., & Lieberman, M. A. (1981). The stress process.Journal of Health and Social Behavior, 22, 337-356. • Pearlin, L. I., & Schooler, C. (1978). The structure of coping.Journal of Health and Social Behaviour, 19, 2-21. • Pearlin, L. I., & Skaff, M. M. (1996). Stress and the life course: A paradigmatic alliance.Gerontologist, 36, 239-247. • Turner, R. J., & Noh, S. (1988). Physical disability and depression: A longitudinal analysis.Journal of Health and Social Behaviour, 29, 23-37.