Download
1 / 97
990 likes | 1.66k Vues
Measles and Other Childhood Exanthems. Donald McLaren, MD Seventh International Symposium in Continuing Nursing Education/March 2014. Goals of talk.

E N D
Measles and Other Childhood Exanthems Donald McLaren, MD Seventh International Symposium in Continuing Nursing Education/March 2014
Goals of talk • To highlight measles as a still very important major cause of under 5 mortality in the developing world and discuss diagnosis, complications and treatment • To discuss clinical features, diagnosis, complications and treatment of various childhood exanthems • To point out some other childhood diseases which may present with a rash which you should not miss because they are potentially fatal if not treated early
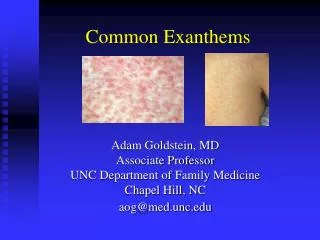
Definitions • Exanthem – widespread rash – from Greek “a breaking out.” A generalized cutaneous eruption associated with a systemic illness • Morbilliform rash – rash that looks like measles. • Macule – discolored area on skin not raised above the service • Papule – raised solid lesion on skin without visible fluid – varies in size but < 5mm
Vesicle – small elevation of epidermis containing serous fluid < 5 mm • Petechiae – very small red spot on skin due to hemorrhage – does not blanch to pressure • Childhood exanthems initially named by number from first to sixth in 1905 - measles, scarlet fever, rubella, 4th never existed, erythema infectiosum, and roseola infantum. • Many other causes of exanthems in children.
Measles (Rubeola) • Prior to vaccine 90% acquired measles by 15 yoa • With high rates of immunization, age in epidemics in U.S shifted downwards to 6 months of age • Still major cause of mortality in developing world. • In 2000, 31-39.9 million got measles with 733,000 – 777,000 deaths (5th in < 5 mortality) • By 2011 mortality dropped by 71% (WHO) • 1990-2008 decreased from 7% to 1% of < 5 mortality! • Van dan Ent M.M.V.X., Brown, DW, Hoekstra, J, Christie A, Cochi SL. Measles Mortality Reduction Contributes Substantially to Reduction of All Cause Mortality Among Children Less than Five Years of Age, 1990-2008. JID 2011:204 (Supplement 1)
Epidemiology • 1990-2008 decreased from 7% to 1% of < 5 mortality! • Van danEnt M.M.V.X., Brown, DW, Hoekstra, J, Christie A, Cochi SL. Measles Mortality Reduction Contributes Substantially to Reduction of All Cause Mortality Among Children Less than Five Years of Age, 1990-2008. JID 2011:204 (Supplement 1) • Goal of 95% reduction over 2000 by 2015 and elimination in 5 WHO regions by 2020 • Africa – 2001-8 vaccination rate 57-73% • SE Asia – 2000-2008 46% reduction in measles deaths • > 70% decreased mortality 2000-2007. 197,000 in 2007 • 85% measles mortality now in Africa, SE Asia
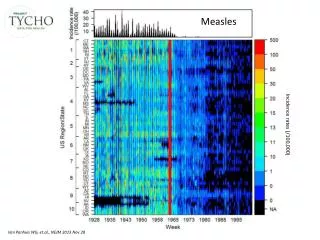
Measles epidemiology • Highly contagious – 75% attack rate if exposed • U.S. pre-vaccine: 500,000-4,000,000 cases/year; 48,000 hospitalized; 1000 chronically disabled; 500 deaths – No longer endemic. • 2001-2011 63 cases/year reported – most 220. 88% import (travel) related and 66-85% of unvaccinated or unknown status. • Outbreak = 3 or more cases linked in time and place
Incidence of global measles 2004http://dualibra.com/wp-content/uploads/2012/04/037800~1/Part%207.%20Infectious%20Diseases/Section%2015.%20Infections%20Due%20to%20RNA%20Viruses/185.htm
http://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/big_measlesreportedcases6months_PDF.pdfhttp://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/big_measlesreportedcases6months_PDF.pdf
Clinical Manifestations of Classic measles • Incubation period: asymptomatic 8-10(6-19) days • Prodrome: Fever, malaise, anorexia • Followed by the 3 Cs.Conjunctivitis, coryza, cough – photophobia. 2-3 days. Fever as high as 400 • Koplick spots (pathognomonic) often appear 48 hours before rash. 1-2 mm whitish or gray elevations on erythematous base in buccal mucosa and other parts of mouth like “grains of salt on a red background”
Exanthem: Maculopapular blanching rash • Starts on face then moves downward and outward • Often become confluent. • Usually spares palms/soles - Occasionally petechial • Lymphadenopathy, high fever, respiratory signs, pharyngitis, nonpurulent conjunctivitis. • Improvement within 48 hours with rash disappearing in same order as appearance • Darkens to brown color after 3-4 days and fades followed by fine desquamation. Lasts 7 days.
Recovery, immunity. Cough up to 2 weeks. • Fever beyond day 4 of rash means complication • Immunity lifelong and reinfection rare. • Contagious 5 days pre-rash to 4 days after rash appears • Anergy not uncommon for several weeks after measles (meaning PPD unreliable)
Measles Clinical Course Hunter’s Tropical Medicine and Emerging Infections Diseases
Other forms of measles • Modified: Pt. with incompletely protective measles antibody. Similar but milder symptoms, longer 17-21 day incubation period • Atypical: Rare - those immunized with killed virus vaccine used 1963-67. Can be very severe with respiratory distress or mild • Starts with HA, high fever 7-14 days post exposure • Dry cough, pleuretic chest pain, pulmonary/hilar nodular lymphadenopathy • M-P rash 2-3 days later begins on extremities, spreads to trunk • Involves palms, soles and spares upper chest, neck and head • May be purpuric, urticarial, hemorrhagic, accentuated in skin folds
Diagnosis • In context of endemic measles fairly easy with clinical presentation • DDx – many other rashes, but symptoms and progression of rash should usually distinguish • Where there is low measles prevalence should diagnose with paired acute/convalescent sera for anti-measles IgM and IgG - at least fourfold increase in IgG. • IgM present within 3, gone by 30 days post rash • IgG 7 days post rash – peak in 14 days after rash.
Complications • Higher in developing countries: 4-10% • More common in very young and old (< 5; > 20) • More complications with malnutrition, crowding, low vitamin A, immunocompromised, pregnancy • Deaths due to pulmonary (pneumonia and croup) or CNS complications • Morbidities include blindness, malnutrition
Pulmonary complications • Pneumonia, bronchiolitis, LTB (croup), OM • Measles giant cell pneumonia in those who are immunocompromised • 5% get bacterial super-infection most commonly from Staph, Strep, H. flu, or pneumococcus and in one South African study 85% deaths due to viral or bacterial lung infection • Antibiotic prophylaxis MAY decrease incidence of secondary infection. Needs more study.
Neurologic complications • Encephalitis 1 / 1000 cases within days of rash. Most recover but • 25% neurodevelopmental sequela; 15% rapidly progressive fatal • Acute disseminated encephalomyelitis (ADEM) • Demyelinating disease during recovery phase • Autoimmune response within 2 wks of infection or vaccine (F, stiff neck, HA, seizures, mental status changes, paralysis) • 10-20% mortality (frequent residual neurological abnormalities) • SSPE (Subacute Sclerosing Panencephalitis) • Fatal progressive degenerative CNS disease 7-10 years post infection • Increased if measles before age 2 years. • Risk much less with vaccine < 1/12 (1:1,000,000)
Other complications • Eye: measles induced keratitis, vitamin A deficiency, corneal ulceration, 20 herpes simplex or bacterial infection, herbal remedies in eye can lead to blindness • GI: Gingivostomatitis, gastroenteritis, D, hepatitis • Diarrhea, stomatitis often lead to worsening nutritional status • Marasmus or Kwashiokor • Cardiac (myocarditis and pericarditis) • Immune suppression (T cell infection) • During pregnancy – uncommon – NOT a teratogen. May have more severe course. Also increased spontaneous abortion and perinatal mortality.
Treatment • Antipyretics • Fluids • Tx bacterial super-infection, complications • Vitamin A – WHO vs. U.S. recommendation • Especially in young < 2 yoa, complicated measles • Mortality, complications, hospital stay reduced. • One study showed no OVERALL decreased mortality but decreased mortality if under age 2
Role of vitamin A • WHO – 2 doses vitamin A to all children with measles in communities with recognized vitamin A deficiency problem and measles related mortality is > 1%. • Must give within 5 days of rash onset to reduce morbidity and mortality • Why does this reduce mortality? • Most likely damage to epithelial membranes increased with low vitamin A AND • Depression of immune response with low vitamin A
Vitamin A continued • AAP and vitamin A • Age 6 months to 12 years AND hospitalized OR • > 6 mo with immunodeficiency, ophthalmological evidence of vitamin A deficiency, impaired intestinal absorption, significant malnutrition, immigration recently from area with high measles mortality. • Single dose (6-12 mo 100,000; > 12 mo 200,000 IU) • Repeat day 2 and 28 if evidence vitamin A deficiency
http://www.measlesrubellainitiative.org/wp-content/uploads/2013/06/Treating-Measles-in-Children1.pdfhttp://www.measlesrubellainitiative.org/wp-content/uploads/2013/06/Treating-Measles-in-Children1.pdf
http://www.measlesrubellainitiative.org/wp-content/uploads/2013/06/Treating-Measles-in-Children1.pdfhttp://www.measlesrubellainitiative.org/wp-content/uploads/2013/06/Treating-Measles-in-Children1.pdf
Prevention • Vaccine beginning at 12 months of age • As early as 6 months if travelling to endemic area • But must give 2 doses after age 1 • Many foreign countries give at 9 months • MMR vs. MMRV (Slightly greater risk of seizure with MMRV with first dose only) • Very effective – 95% if 1st vaccine at age 12 moa • Second dose at least 28 days later (ACIP) and for sure by school entry at 4-6 years of age
Prevention if exposed • Measles vaccine within 3 days of exposure • Immune globulin if can’t get vaccine, or 3-6 days after exposure, or < 12 months old in household • SE vaccine: Fever (5-15%) or transient rash (5%) 1-2 weeks later; NO autism association • If refuse vaccine – exclude from setting for 3 weeks after onset of rash of last measles case
Scarlet Fever or Scarlatina • Diffuse erythematous eruption usually associated with strep pharyngitis and following it by 12-48 hours • Due to delayed – type skin reactivity to pyogenic exotoxin from Group A (B and C) streptococci • Rash: • diffuse blanching erythema • Numerous small 1-2 mm papular elevations giving rise to sandpaper feel to skin • Starts head/neck with circumoral pallor , strawberry tongue • Extends to trunk then extremities • Ultimately desquamates.
Most marked at skin folds of inguinal, axillary, antecubital and abdominal areas, pressure points. • Pastia’s lines – petechia in antecubital fossa and axillary folds. • Treatment – antibiotics: Penicillin, Amoxicillin or Ampicillin, erythromycin, cephalosporins • Isolate till 24 hours after antibiotics started
Rubella (“German Measles”) • Three day measles. Initially thought to be measles or scarlet fever variant. • Described 1750s in Germany • Named rubella in 1866 • Interest increased when Australian eye doctor described teratogenic effects on the eye in 1941 • Prior to good vaccine up to 12 million cases in 1964-65 with 20,000 CRS (Congenital rubella syndrome) cases • Pre-vaccine (1969) 58 cases/100,000. 1983 ↓ to 0.5 / 100,000. Eliminated from U.S. (2004); Americas (2010)
Clinical Course of Rubella • Incubation 14-18 days (12-23) after inhalation of particulate aerosols • Contagious 1-2 wks before clinical recognition • Viral shedding decreases with appearance of rash but contagious till a week after rash • Re-infection possible but rarely leads to CRS
“Rubella is a mild disease with clinical features that are neither distinctive nor diagnostic.”Hartley AH and Rasmussen JE. “Infections Exanthems.” Pediatrics in Review accessed online a http://pedsinreview.aappublications.org/content/9/10/321
Signs/symptoms • Usually mild and often asymptomatic • Acute onset M-P rash - few systemic symptoms • Rash erythematous, nonpruritic, discrete • Low grade fever, lymphadenopathy concurrently or 1-5 days prior to rash • Lymphadenopathy – posterior cervical, posterior auricular, suboccipital • Spreads face to trunk, extremities – fading on face by day 2
Generalized within 24 hours, gone within 3 days (1-8) without peeling or scaling. Much more rapid than measles; does not darken or coalesce • Teens, adults – more likely to be more symptomatic with fever, systemic complaints. Arthralgias, arthritis in 70% lasting up to a month – knees, wrists, fingers • Complications more common in adults – postinfectious encephalitis (1 in 6000 within week): immune mediated and good prognosis OR progressive rubella panencephalitis (rare and devastating)
Congenital Rubella Syndrome • Real concern with Rubella is CRS – hearing loss, MR, CV defects, ocular defects • CRS highly variable but any organ system can be effected. Can manifest throughout life. • Vaccine effective; goal of immunization to prevent CRS (25% transient arthralgia; 10% arthritis after vaccine) • Rubella still a big deal in third world
Congenital rubella syndrome • Highest risk first 10 weeks of gestation – Unlikely if after 18-20 weeks. 80% risk first trimester • Consider in any birth if rubella during pregnancy or any infant with IGR or other findings c/w CRS • Children can shed virus after CRS at least a year • Dx of rubella unnecessary except when CRS suspected. Cord blood IgM or persistence of IgG beyond 1st year of life (normally disappears at 3-6 weeks)
Erythema Infectiosum or Fifth disease • Mild febrile disease with rash: caused by Parvovirus B19 infection • Five forms of B19 infections which also causes • Arthropathy • Non-immune hydrops fetalis with Intrauterine fetal death or miscarriage • Transient aplastic crisis in chronic hemolytic disorders • Chronic pure RBC aplasia in the immunocompromised
Signs/symptoms • Incubation period 4-14 days – biphasic illness • 25% asymptomatic, 50% flu like symptoms, 25% classic presentation including rash. • First week viremia with non-specific flu like illness (fever, malaise, myalgia, coryza, HA, pruritis) • Can have low platelets, Hgb, or leukopenia • Next week rash and/or arthralgia • In adults less characteristic - can be confused with rubella
Fifth disease outbreaks among school age children • Nonspecific prodromal symptoms (Fever, coryza, HA, N, D) • 2-5 days later classic erythematous malar rash (slapped cheek appearance)relative circumoral pallor • Followed by reticulated (lacelike) rash on trunk, extremities • Viremia has resolved and child feels well by time rash appears (rash felt to be immune mediated)