Download
1 / 29
310 likes | 466 Vues
Explore the roles, regulation, and clinical significance of bicarbonate and magnesium in the body's metabolic processes. Learn about their assay methods, regulation mechanisms, and clinical implications.

E N D
Electrolytes Part 2
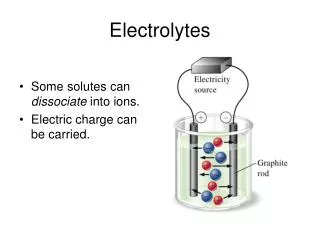
Bicarbonate • 2nd most abundant anion of ECF. • Major component of the HCO3-/H2CO3 buffering system. • Serves as a transport form for CO2 produced from metabolic processes in tissues • HCO3- accounting for more than 90% of the total CO2 at physiologic pH • Total CO2 measurement is indicative of HCO3- measurement M. Zaharna Clin. Chem. 2009
Bicarbonate • Carbonic anhydrase in RBCs converts CO2 and H2O to carbonic acid, which dissociates into H+ and HCO3-. • HCO3- diffuses out of the cell in exchange for Cl- to maintain ionic charge neutrality within the cell (chloride shift) • This process converts potentially toxic CO2 in the plasma to an effective buffer: HCO3- • HCO3- buffers excess H+ by combining with acid, then eventually dissociating into H2O and CO2 in the lungs where the acidic gas CO2 is eliminated. M. Zaharna Clin. Chem. 2009
Regulation • Bicarbonate conc. is regulated both in: • Kidneys through increased or decreased tubular reabsorption • And in lungs through exhalation of gaseous CO2 and H2O • Decreased levels of HCO3- in plasma result in acid-base disorder (acidosis) • Increased levels result in alkalosis M. Zaharna Clin. Chem. 2009
Alkalosis & Acidosis • In alkalosis, • a relative increase in HCO3- compared to CO2, • the kidneys increase excretion of HCO3- into the urine, • carrying along a cation such as Na+. • This loss of HCO3- from the body helps correct pH. • In acidosis • The body increases excretion of H+ into the urine. • In addition, HCO3-reabsorption is virtually complete, with 90% of the filtered HCO3- reabsorbed in the proximal tubule and the remainder in the distal tubule. M. Zaharna Clin. Chem. 2009
Assay • Two common methods: • Ion selective electrode • Enzymatic: • converts all forms of CO2 to HCO3; • HCO3 is used to carboxylate phosphoenolpyruvate. • Coupled enzyme reaction that measures the amount of NADH consumed. • The rate of absorbance change is proportional to amount of CO2 present. M. Zaharna Clin. Chem. 2009
Magnesium • 4th most abundant cation in the body and 2nd most abundant intracellular cation. • 53 % of Mg found in the bone, 46 % in muscle and tissue, <1% is present in the serum & RBCs. • The Mg circulating in serum • one third-bound to albumin, • of the remaining two thirds- • 61% is in the free or ionized form, • 5 % bound to phosphate and citrate. • Free form is physiologically active. M. Zaharna Clin. Chem. 2009
Regulation of Magnesium • Regulated by dietary intake, intestine may absorb 20-65 % of dietary intake and body needs. • Regulation of body Mg2+ is controlled largely by the kidney, which can: • reabsorb Mg2+ in deficiency states • or readily excrete excess Mg2+ in overload states 2%-5% is reabsorbed in the DCT 25%-30% is reabsorbed by PCT 50%-60% of filtered Mg2+ is reabsorbed in Henle's loop M. Zaharna Clin. Chem. 2009
Regulation of Magnesium • Mg2+ regulation is related to that of Ca2+ and Na+. • Parathyroid hormone (PTH) increases the renal reabsorption of Mg2+ and enhances the absorption of Mg2+ in the intestine. • Aldosterone and thyroxine apparently have the opposite effect of PTH in the kidney, increasing the renal excretion of Mg2+ M. Zaharna Clin. Chem. 2009
Clinical Significance • Roles in the body: • Myocardial rhythm and contraction • It is an essential cofactor of more than 300 enzymes, • Regulation of ATPase ion pump • Abnormal levels related to cardiovascular, metabolic, and neuromuscular disorders. M. Zaharna Clin. Chem. 2009
Hypo- & Hypermagnesaemia • Hypomagnesaemia: • Reduce intake • Decreased absorption (GI disorders, Malabsorption syndromes) • Increased excretion (as a result of various renal and endocrine disorders) • Hypermagnesaemia: • Decreased excretion (Adrenal insufficiency ) • Increased intake M. Zaharna Clin. Chem. 2009
Assay • Methods (colormetric) • Calmagite • Mg2+ binds with calmagite to form a reddish-violet complex • Formazan dye • Mg2+ binds with the dye to form a colored complex • Methylthymol blue • Mg2+ binds with the chromogen to form a colored complex • Reference Range : 0.63-1.0 mmol/L M. ZaharnaClin. Chem. 2009
Calcium • 99 % of calcium is associated with bone tissue • Only 1 % of body calcium is in the plasma • 45 % ionized (active form) • 40 % protein bound • 15 % bound to other compounds • Critical component of cardiac function • Decreased ionized Ca2+ concentrations in blood can cause neuromuscular irritability M. Zaharna Clin. Chem. 2009
Regulation • Three hormones, PTH, vitamin D, and calcitonin, are known to regulate serum Ca2+ by altering their secretion rate in response to changes in ionized Ca2+. • Decreased plasma ionized Ca stimulates release of PTH • PTH activates a process known as bone resorption • PTH increases renal reabsorption of Calcium • PTH stimulates Vitamin D activation • Vitamin D increases GI absorption of Calcium • Calcitonin exerts its Ca2+-lowering effect by inhibiting the actions of both PTH and vitamin D M. Zaharna Clin. Chem. 2009
Regulation osteoclasts M. Zaharna Clin. Chem. 2009
Clinical Applications • Both total Ca2+ and ionized Ca2+ measurements are available in many laboratories, • Ionized Ca2+ is usually a more sensitive and specific marker for Ca2+ disorders. • Causes of hypocalcemia • Hypoparathyroidism • Vitamin D deficiency • Renal disease • Hypoalbuminemia (total calcium only, ionized not affected) M. Zaharna Clin. Chem. 2009
Clinical Applications • Causes of hypercalcemia • Hyperparathyroidism • Malignancy (many tumors produce PTH-related peptide (PTH-rP), which binds to normal PTH receptors • hyperthyroidism can sometimes cause hyperparathyroidism because of the proximity M. Zaharna Clin. Chem. 2009
Assay Methods • The two commonly used methods for total Ca2+ analysis which form a complex with Ca2+ use either: • ortho-cresolphthaleincomplexone (CPC) • or arsenzo III dye • Adult reference range: 8.6-10.0 mg/dL M. Zaharna Clin. Chem. 2009
Phosphate • Element found everywhere in living cells • Participates in various biochemical processes • Most significant: ATP, Creatine Phosphate, phosphoenolpyruvate reactions. • Important compound in the release of O2 from Hb (2,3-diphosphoglycerate) • (DNA) and ribonucleic acid (RNA) are complex phosphodiesters M. Zaharna Clin. Chem. 2009
Phosphate • The concentration of all phosphate compounds in blood is about 12 mg/dL • most of that is organic phosphate • and only about 3 to 4 mg/dL is inorganic phosphate. • Phosphate is the predominant intracellular anion, with intracellular concentrations varying, depending on the type of cell • less than 1% is active in the serum/plasma M. Zaharna Clin. Chem. 2009
Regulation • Phosphate in blood may be: • absorbed in the intestine from dietary sources, • released from cells into blood, • and lost from bone. • In healthy individuals, all these processes are relatively constant and easily regulated by: • renal excretion • or reabsorption of phosphate. M. Zaharna Clin. Chem. 2009
Regulation • Renal regulation is effected by factors such as: • Vitamin D, • increases both phosphate absorption in the intestine and phosphate reabsorption in the kidney • PTH, • lowers blood concentrations by increasing renal excretion. M. Zaharna Clin. Chem. 2009
Clinical Application • Hypophosphatemia: • Intracellular shift • Hyperparathyroidism • Renal tubular defect • Hyperphosphatemia: • Increase intake • Decrease excretion • Cell lysis M. Zaharna Clin. Chem. 2009
Assay Methods • Most of the current methods involve the formation of an ammonium phosphomolybdate complex. • This colorless complex can be measured by ultraviolet absorption at 340 nm • or can be reduced to form molybdenum blue, a stable blue chromophore, which is read between 600 and 700 nm. • Adult reference range: 2.4-4.4 mg/dL M. Zaharna Clin. Chem. 2009
Anion Gap • Body water compartments exist in a state of electroneutrality (anions=cations) • Routine measurements: Na, K, Cl & HCO3 levels • Anion Gap is the difference between unmeasured anions and unmeasured cations. • Formula: AG=(Na + K)- (Cl + HCO3) • The "real" balance is given by the equation: [Na]+ [K] + [other cations] = [Cl] + [HCO3] + [other anions] ([Na]+ [K]) - ([Cl] + [HCO3])= [other anions] - [other cations] = "Anion Gap“ M. Zaharna Clin. Chem. 2009
Anion Gap • Some of the unmeasured cations (~7mmol/L) include calcium, magnesium, and most other minerals. • Unmeasured anions (~24 mmol/L) include proteins like albumin, and phosphates, sulfates, etc. • There are always more unmeasured anions than cations, and thus the "anion gap" equationis always greater than zero. • It has a reference range of 10-20 mmol/L M. Zaharna Clin. Chem. 2009
Clinical Uses of the Anion Gap • An elevated anion gap may be caused by: • uremia/renal failure, which leads to PO4- and SO42- retention; • ketoacidosis, as seen in cases of starvation or diabetes; • methanol, ethanol poisoning • and instrument error. • Low anion gap values are rare but may be seen with: • hypoalbuminemia (decrease in unmeasured anions) • or severe hypercalcemia (increase in unmeasured cations). M. Zaharna Clin. Chem. 2009