The Kidney in Pregnancy
430 likes | 761 Vues
The Kidney in Pregnancy. Jeffrey J. Kaufhold, MD FACP Update 2010. Renal Physiology. Overview of Physiology 101 Nitric Oxide Physiology Endothelin Physiology Normal Changes in Pregnancy Pathophysiology in Pregnancy. Glomerular Physiology Blood flow determinants. Systemic. AT-II ANS.

The Kidney in Pregnancy
E N D
Presentation Transcript
The Kidney in Pregnancy Jeffrey J. Kaufhold, MD FACP Update 2010
Renal Physiology • Overview of Physiology 101 • Nitric Oxide Physiology • Endothelin Physiology • Normal Changes in Pregnancy • Pathophysiology in Pregnancy.
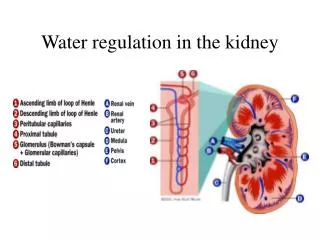
Glomerular PhysiologyBlood flow determinants Systemic AT-II ANS Afferent Efferent PG's Local TGF Filtration
Renal Physiology 201 • Explosion of Research in NO and ET • In the last 4 years, over 3000 publications each.
Nitric Oxide • Functions: • Regulate BP • Neurotransmitter • Suppress Pathogens • Studies describe Pathophys. in: • Pregnancy/Pre-ecclampsia • HTN • Hepatic Failure
Endothelin • Function: • Most potent vasoconstrictor • Studies describe broad range of Pathophysiologic conditions.
Why is this Important? • Inhibitors and Antagonists being developed which you will use soon • You already use some: • Nitroprusside • Isordil/NTG • Viagra
Nitric Oxide - NO • Uncharged molecule - can go anywhere • Unpaired electron - highly reactive • Chemical generation: • Arginine + O2-----> NO + Citrulline NOS
Enzyme Production • Nitric Oxide Synthase (NOS) • Two Types • Constitutive • vasodilator • neurotransmitter • Inducible • Free radical scavenger • Pathogen killer
Targets: Vascular Smooth Muscle Neurons Pathogenic bacteria Effects: Vasodilator Feedback for ET-1 Neurotransmitter Free Radical/Killer Nitric Oxide
Progesterone • Stimulates Nitric Oxide Synthase • See below • Stimulates Relaxin • to soften Ligaments/ allow opening of Birth Canal • Hydroureter • Stimulates Ventilation • Chronic Resp Alkalosis, • Useful in Sleep apnea
Normal Changes in Pregnancy • Systemic Vasodilation • Lower BP • Increased Aldosterone • Volume expansion / edema • Increased GFR / RBF • Angiogenesis
Normal Changes in Pregnancy Chapter 6, part 1, Medical Care of the Pregnant Patient
Glomerular PhysiologyBlood flow determinants Systemic AT-II ANS Afferent Efferent PG's Local Increase Calcium excretion Decrease uric acid reabsorption Due to reduced filtration fraction TGF Filtration
Progesterone • Stimulates Nitric Oxide Synthase • Decreased response to Angiotensin
Progesterone • Stimulates Nitric Oxide Synthase • Leads to systemic Vasodilation • Which causes lower BP, • Which stimulates Aldosterone • Which leads to volume expansion • Which increases GFR/RBF • Decreased response to Angiotensin
NonVascular Functions of NO • Modulates immune response • reduces toxicity of oxygen radicals • reduces adhesion of neutrophils, etc • inhibits mast cell degranulation • Pregnancy is an Immune Tolerant Condition
Pathophysiology • Hypertension • Proteinuria • Pre-ecclampsia • HELLP syndrome • Pre-existing renal disease • Pre-existing Hypertension
Pathophysiology • Hypertension • Proteinuria • Return of Responsiveness to Angiotensin
Pathophysiology • Pre-ecclampsia • Severe HTN with risk for seizures • Vacuole formation in endothelial cells • Circulating Inhibitors of NOS • HELLP syndrome • Hepatic dysfunction due to underperfusion • Low platelets due to fibrin deposition and scything of cells in capillaries • Increased Endothelin
Ecclampsia vacuoles Hyaline thrombus
Pathophysiology • Pre-existing renal disease • General rule is • 1/3 worsen • 1/3 stable • 1/3 improve • Pre-existing Hypertension • Tends to improve • Which drugs to use?
Pathophysiology • Hypertension Which drugs? • First Line: Aldomet, Labetolol • Second Line: Hydralazine, Pindolol, Acebutolol, Nifedipine. • Third Line: Atenolol, Inderal, clonidine, diltiazem, verapamil, HCTZ • Contraindicated: ACE inhibitors
ENDOTHELIN • Three Types • Produced by endothelial cells, most renal cell types. • Two receptor types, A and B
ENDOTHELIN • Stimulators: • Vasoconstrictors • Thrombin • Hypoxia • Low shear stress • Cytokines
ENDOTHELIN • Inhibitors of production • Vasodilators • Heparin • High shear stress
ENDOTHELIN • Feedback inhibition by Nitric Oxide, PGI2 (prostacyclin) • Also inhibited by activation of ET-B receptor on the endothelial cell
Vascular Smooth M. Renal Tubules Mesangial cells Vasoconstriction Sodium excretion Proliferation, accumulation of Matrix, and contraction. ENDOTHELIN Effect Target
ENDOTHELINClinical Aspects • ATN • Contrast nephrotoxicity • Cyclosporine nephrotoxicity • Endotoxic shock • Hypertension • Chronic renal failure
Clinical Aspects of N.O. • Cirrhosis • decreased BP, low SVR, angiogenesis • NOS inhibitors work, sort of. • Pregnancy • reduced response to angiotensin • natural inhibitor found in pre-ecclampsia
Pre-eclampsia Mediators • Soluble fms-like Tyrosine Kinase-1 • sFLT1 • Antagonizes VEGF, Placental Growth Factor (PlGF) • Soluble Endoglin • sENG • Cleavage product of TGF-B receptor • Maynard SE, Thadani R. Pregnancy and the Kidney. JASN Vol 20, 2009, p 14-22.
Pre-eclampsia Mediators • Autoantibodies to Angiotensin I receptor • Found in pre-eclampsia and other condiitions • May play a role but are not specific • Deficiency of Catechol-O-Methyl Transferase (COMT) placental enzyme which breaks down catecholamines. • Maynard SE, Thadani R. Pregnancy and the Kidney. JASN Vol 20, 2009, p 14-22.
Future Markers for Pre-eclampsia • Placental Protein 13 (PP13) • Placental artery doppler in 3rd trimester • Genetic predisposition with certain Gene markers • Uric Acid level increases. Why? • Maynard SE, Thadani R. Pregnancy and the Kidney. JASN Vol 20, 2009, p 14-22.
Glomerular PhysiologyBlood flow determinants Systemic AT-II ANS Afferent Efferent PG's Local Due to increased filtration fraction Reduce Calcium excretion Increase uric acid reabsorption TGF Filtration
Future Treatments for Pre-eclampsia • VEGF • Vascular Endothelial Growth Factor • L-arginine • Substrate for Nitric Oxide Synthase • Maynard SE, Thadani R. Pregnancy and the Kidney. JASN Vol 20, 2009, p 14-22.
Summary • Physiology and Pathophysiology of • Nitric Oxide • Endothelin • Physiology and Pathophysiology of the kidney in Pregnancy
References • Medical Care of the Pregnant Patient • RV Lee, K Rosene-Montella et al. Published by the American College of Physicians (acponline.org), 2000 • Kidney Disease and Pregnancy • Dr Phyllis August • www.kidneyatlas.org/book4/adk4-10.pdf • Pregnancy Outcomes after kidney Donation • www.nephrologynow.com/publications/pregnancy-outcomes-after-kidney-donation • Ibrahim et al. Am J Transplant. 2009 Apr;9(4):825-34 • Maynard SE, Thadani R. Pregnancy and the Kidney. JASN Vol 20, 2009, p 14-22.