Download
1 / 14
200 likes | 570 Vues
Reabsorption In the Kidney. Objectives. Describe the general structure of the kidney , the nephron , and associated blood vessels Explain the functioning of the kidney in the control of water by ADH and in the excretion of metabolic waste. Where Were We?.

E N D
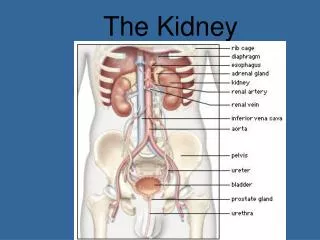
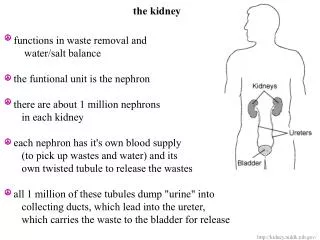
Objectives • Describe the general structure of the kidney, the nephron, and associated blood vessels • Explain the functioning of the kidney in the control of water by ADH and in the excretion of metabolic waste
Where Were We? The removal of an amino group from amino acids that forms ammonia. Ammonia is converted to urea by combining with CO2 • What is deamination? What happens to ammoina? • What is the pathway of waste material from the liver to outside the body? • What is a glomerulus and renal capsule? • What keeps ultrafiltration rates so high? Liver blood plasma afferent arterioleglomerulus renal capsule proximal convoluted tubule Loop of Henle distal convoluted tubule collecting ductsureter bladder urethra outside the body Glomerulus spliting of capillaries in renal capsule to increase filtration rate Renal capsule site of blood filtration in the nephrons of the kidneys; cup-shaped High pressure in glomerulus caused by the wide afferent arteriole and narrow efferent arteriole keeps a high water potential inside glomerulus so materials diffuse out quickly
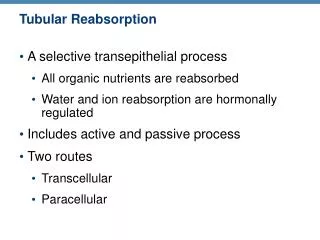
Reabsorption: 4 Areas • Selective reabsorption pulling materials required for homeostasis back into the blood through the nephron • Proximal convoluted tubule • Main site of reabsorbtion; 65% H2O • Pulls out all glucose and most amino acids, vitamins, and minerals • Loop of Henle • Raises salts levels in tissue fluid so water can be absorbed quickly • Distal convoluted tubule • Pulls out water, Na+ and pulls in K+ • Collecting ducts • Pulls out water, Na+ and pulls in K+
Proximal Convoluted Tubule • Filtrate is full of useful material: • Glucose • H2O • Ions (Na+, Cl-, K+) • Epithelial cells on tubule is lined with microvilli, filled with mitochondria, and are ready for lots of active transport and diffusion • Basic actions: • Na+ ions actively pumped(Na+/K+ pump) from epithelial cells into blood • causes diffusion of Na+ into epithelial cells • Na+ movement pulls in glucose, vitamins, and minerals into epithelial through co-transport proteins • Glucose, vitamins, and minerals diffuse into blood
PCT lumen Blood vessel ATP Na+ ADP +Pi ATP Na+ Na+ ADP +Pi Glucose ATP Na+ Na+ Vitamins ADP +Pi Na+ Amino acids
PCT lumen Blood vessel Na+ concentration gradient Na+ Glucose Na+ Vitamins Na+ Amino acids
PCT lumen Blood vessel Na+ Glucose Na+ Vitamins Na+ Amino acids
Proximal Convoluted Tubule • Glucose, vitamins, and minerals diffuse into the blood. What does this do to the solute conc. in the filtrate? • Drops dramatically • So what happens to H2O if the solute conc. is increasing in the blood? • Move by osmosis into the blood • 65% of the 125 cm3 filtrate is absorbed back into the blood • 85% H2O is reabsorbed • 55% of urea slips back into blood
Loop of Henle • Reabsorption through a two limb system • Descending Limb • Permeable to H2O and Na+/Cl- • H2O drawn out by osmosis due to high Na+ and Cl- conc. • Na+ and Cl- drawn in by diffusion • Ascending Limb • Impermeable to H2O and Na+ • Actively pump Na+ and Cl-out of the limb; 4x normal conc. • Bottom of loop high ion/ low water • Top of loop low ion/high water
Descending side Ascending side 2) Because of the high ion conc. outside, water is drawn into tissue fluid by osmosis 1) Ions are pumped into the tissue fluid around the loop
Descending side Ascending side • Counter-current Multiplier • Fluid in both limbs reinforce the tissue fluid and the limbs have the maximum ion concentrations 3) Ions diffuse down a conc. gradient into the descending side 4) As water leaves, bottom of loop becomes very conc. with ions 5) Lower parts of ascending loops are conc. enough for Ions to diffuse out Salt concentration
Distal Convoluted Tubules • What is the conc. of filtrate leaving the Loop of Henle? • Low ion conc. so has a high water potential • How will water in the filtrate move? • Drawn into tissue fluid by osmosis • Na+/K+pumps remove Na+ from filtrate and add K+ to filtrate based on blood ion conc.
Collecting Ducts • What is the tissue fluid conc. like in the medulla? • High ion conc. from the Loop of Henlecounter-current multiplier • What happens to the filtrate as it passes through the collecting ducts in the medulla? • Water absorbed into tissue fluid (and blood) through osmosis • Urine becomes more conc. until it matches that of the tissue fluid • Na+/K+ pumps regulate Na+ and K+ conc. in tissue fluid and urine • Controlled by ADH (antidiuretic hormone)