
STOMACH AND DUODENUM
E N D
Presentation Transcript
STOMACH AND DUODENUM Chapter 13
STOMACH AND DUODENUMObjectives • Anatomy and Physiology • Peptic Ulcer Disease • Zollinger Ellison Syndrome • Neoplasms
AnatomySTOMACH • Four regions • Cardia, Fundus, Antrum, Pylorus • Parietal cells, Chief cells, Antral G cells, Mast cells • Blood supply • Gastric and gastroepiploic arteries • short gastrics and gastroduodenal • Innervation • Vagus
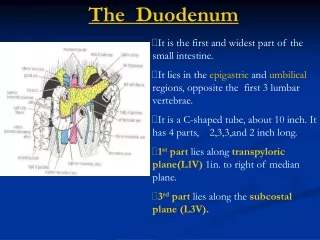
AnatomyDUODENUM • Four regions • Bulb, Descending, Transverse, Ascending • Blood supply • Mainly from gastroduodenal artery
Physiology • Acid Secretion • Parietal Cell • acetylcholine, gastrin, histamine • Cephalic phase- sight/smell, vagal • Gastric phase- antral distention, gastrin • Intestinal phase- histamine • Inhibition of gastric acid • Secretin • Somatostatin
Acute Ulcer Disease • Most common in 1st portion of duodenum and lesser curvature of the stomach • Burning epigastric pain • Duodenum- relieved by food • Stomach- produced by food • Upper GI bleed • Acute abdomen • gastric outlet obstruction • Diagnosis • history • Upper GI series • Endoscopy
Acute Ulcer DiseaseTreatment • Upper GI Bleed • NGT, Large IV’s, Resuscitation, antacids/H2 Blockers, Endoscopy • Surgery- if > 6 U of blood or if remains unstable • Perforation- Exp Lap • Graham’s patch • Acid reducing procedure • Gastric outlet obstruction • NGT, IVF, Correct electrolyte abnormalities • Surgical inervention if necessary
Chronic UlcerTreatment • Conservative medical treatment • Diet- avoid caffeine, alcohol, chocolate • H2 blockers • Proton pump inhibitors • H. Pylori eradication- 2 weeks of triple therapy • Surgical • Truncal vagotomy and pyloroplasty • Selective vagotomy and pyloroplasty • Proximal gastric vagotomy • Antrectomy- Billroth I and II • For gastric ulcers be suspicious for cancer
Zollinger Ellison Syndrome • Gastrinoma- gastrin producing tumor • 60% are malignant- slow growth pattern • Associated with MENS I • Present with refractory PUD. • Diagnosis- • fasting gastrin serum >300 • Secretin infusion test • Treatment • Medical • Surgical excision
Gastric Carcinoma • Epidemiology- Geographic and diet • Presentation- Usually Asx. • Bloating, wt loss, melena, + hemoccult • Pathophysiology • All gastric CA are adenocarcinomas • Polypoid, ulcerating, linitis plastica • Metastasis through lymph nodes • Diagnosis • Upper GI Series • Endoscopy andbiopsy • CT Scan
Gastric Carcinoma • Treatment • Surgical Resection- subtotal gastrectomy and gastrojejunostomy vs. total gastrectomy • 5 year survival of 10% • Palliation • Chemoradiation- no survival benefit