Download
1 / 74
750 likes | 931 Vues
STI Prevention in Adolescents and Long-Acting Reversible Contraceptives (LARC). Fareeda Haamid, DO, FAAP Nationwide Children’s Hospital Section of Adolescent Medicine The Ohio State University Assistant Professor of Clinical Pediatrics. STI Prevention . STI Prevention Methods.

E N D
STI Prevention in AdolescentsandLong-Acting Reversible Contraceptives(LARC) Fareeda Haamid, DO, FAAP Nationwide Children’s Hospital Section of Adolescent Medicine The Ohio State University Assistant Professor of Clinical Pediatrics
STI Prevention Methods Not Sexually active Sexually active Vaccine Condoms Mutual monogamy Fewer sex partners Tested Treatment (partner too) • Vaccine • Abstinence
Sources of info for adolescents • Parents • Peers • Sex education • Media • Medical community
STI Prevention MethodsProvider strategies • Medical Providers • Public Health • Social Work • Training • Clinical Practice • Research
Who do you think you’re talking to? Knowing your patient population
Developmental Stages of Adolescence • Early Adolescence: 10-13 years • Middle Adolescence: 14-16 years • Late Adolescence: 17-21 years
Developmental Tasks of Adolescence(what they need to do become adults) • Cognitive Tasks • Psychosocial Tasks • Physiologic Tasks • Puberty and Growth Spurt
Cognitive (what the brain has to do)
The Adolescent BrainCognitive Tasks • Frontal lobe • impulse control • planning • organizing • strategizing • other executive functions • Develops into the 20’s • Role in how they process info
Cognitive Tasks Puberty stage not always = cognitive development stage Concrete thinking formal operational thinking Abstract/symbolic thinking increases Egocentrism “Imaginary Audience”:everyone’s looking at me Feeling invincible/immortal Consider long-term consequences of actions
Psychosocial (how they interact with society/others)
Psychosocial Tasks Main task is development of identity Preoccupation with their appearance Separation from parents/parental influence Increasing importance of peer group Exploration and definition of independence-dependence boundaries Family still primary nurturing & protective source
Protective Factors • Individual or environmental characteristics, conditions, or behaviors that reduce the effects of stressful life events • School connectedness • Parental monitoring • Resilience • Positive peer influences
Teen Rankings Of Top 31 Items Influencing The Decision To Seek Health Care • Providers wash hands • Providers use clean instruments • Providers are honest with patients • Providers and staff are respectful • Providers and sites are clean Ginsburg, et al, JAMA 1995
“10 Things Doctors Do Wrong”A Teen Perspective: • Doctors seem to care more about my insurance information than about my pain. • They act like my time doesn’t count. They should apologize when they’re running late! • They act like they know me when they only know my chart. • Doctors talk to my parent and not to me. • ...I don’t understand what they said. Himelstein, 2012 (Healthy Kids Blog)
“They only know my chart” • Jot down an interesting fact about the patient • Favorite musician • Position they play on a team • Ask their hobbies • Ask their fears
“I don’t understand what they said” • They’re not stupid…they just don’t think like you do • Ask them to repeat a key item discussed • How would you explain what I said to your friends? • Use very plain language for written instructions • After visit summary (AVS) • Discharge Instructions
“They talk to my parent and not to me” • Teens receive better care when they know that confidentiality will be maintained • Assurances of confidentiality have been shown to increase teens’ willingness to discuss sensitive info
Confidentiality • All the major American medical organizations support the provision of confidential care for adolescents (AAP, AMA, SAHM, AAFP, ACOG) • The AAP and AMA recommend seeing patients alone for part of the visit starting at age 11 or 12 • Essential component in the improvement of adolescent health services nationally (IOM 2009)
Confidentiality Rationale • Protects the health of adolescents and the public • Some adolescents forego care if no confidentiality • Most sexually active teen girls would stop, delay or d/c using specific health services if parents were notified • Planned Parenthood study: Reddy et al JAMA 2002 • Male adolescents: privacy concerns are a main barrier to care Linburg et al Compr Pediatr Nurs 2006 • Impacts willingness to follow up
Confidentiality • In the time spent with just the teen: • Ask again if they have any concerns • Talk about something other than their diagnosis • Praise them for healthy behaviors • Reinforce safe behaviors
Long-Acting Reversible Contraceptives(LARC) Birth control options for adolescents and young adults
Percentage of High School Students Who Were Currently Sexually Active,* 1991 – 2011† * Had sexual intercourse with at least one person during the 3 months before the survey. † Decreased 1991-2011, p < 0.05. National Youth Risk Behavior Surveys, 1991–2011
Adolescent Contraceptive Use % of all contracepting U.S. women ages 15-19 by method type
Adolescent Unintended Pregnancy 82% Unintended 1/5 of all unintended pregnancies in the U.S.
National Teen Birth Rates 1940-2010(births per 1,000 girls aged 15-19) 31.3 (2011) NCHS
2011: The latest data • Live birth rate for 15-19 yo: 31.3 per 1000 • Lowest birth rate ever recorded FOR THIS AGE GROUP • Rates fell steeply 2007- 2011 • Overall rate declined 25% • Reasons: less sexually active, ↑ preventative measures • 23% YRBSS youth reported that either they or their partner had used contraception before last sexual intercourse NCHS, Hamilton (May 2013) and National Youth Risk Behavior Study (2011)
Review of various birth control methods How good are they at preventing pregnancy?
Percentage of women experiencing an unintended pregnancy during the first year of contraceptive use Effectiveness Group Family Planning Method Typical-Use Perfect-Use No Method No method 85% 85% Male latex condoms 15% 2% Less effective Diaphragm 16% 6% Female condoms 21% 5% Spermicide 29% 18% Withdrawal 27% 4% Fertility Awareness 25% 3-5%
Percentage of women experiencing an unintended pregnancy during the first year of contraceptive use Effectiveness Group Family Planning Method Typical-Use Perfect-Use Birth control pills 8% 0.3% Effective Transdermal patch 8% 0.3% NuvaRing® 8% 0.3% Trussell J. Contraceptive Technology 2007.
Percentage of women experiencing an unintended pregnancy during the first year of contraceptive use Effectiveness Group Family Planning Method Typical-Use Perfect-Use Female sterilization 0.5% 0.5% Nexplanon® (progestin implant) 0.05% 0.05% Highly Effective (for all users) Depo Provera 3% 0.3% Mirena® (LNG-IUD) 0.2% 0.2%
Increased use of LARChas the potential to lower unintended pregnancy rates among adolescents
CHOICE Study rationale: • Eliminate barriers: access and cost • Provide brief counseling that focuses on efficacy • Trust each woman to pick the best method for her unique needs
What we learned about LARC… • CHOICE adolescents overwhelmingly picked LARC • 69% of 14-17 year olds (63% implant, 37% IUD) • 61% of 18-20 year olds (29% implant, 71% IUD) Mestad, R, et al. Contraception 2011
What we learned about LARC… • Highest rates of satisfaction and continuation of all reversible methods • 81% continuation rate at 1 year vs. 53% discontinue rate for non-LARC methods • Same rate of continuation as older women Rosenstock, JR, et al. Obstetrics and Gynecology 2012
What we learned about LARC… • 20 times more effective than combined hormonal methods • CHOICE teen birth rate was 1/5 the national rate • 6.3/1,000 vs. 34.3/1,000 • Abortion rates in CHOICE were less than half the regional and national rates Winner, B, et al. NEJM 2012 Peipert, J, et al. Obstetrics and Gynecology 2012
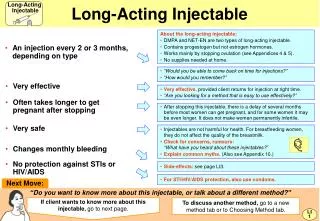
LARC methods… • All require that providers are trained to insert them • All are progestin-only methods (contain no estrogen)
Breastfeeding • Copper IUD has no effect on breastfeeding • Hormonal content of LNG IUS raises theoretic concern • No difference found in breastfeeding duration or infant growth between Copper IUD and LNG IUS users
LARC methods… NEXPLANON®
Previously known as Implanon® Nexplanon®
Nexplanon® • The most effective contraceptive method • Effectiveness: 99.9% • Effective for up to 3 yrs • Progestin-only method: Etonogestrel 68 mg • 4 cm rod (size of a match stick) • No future impact on fertility
Mechanism of action:How does it prevent pregnancy? • Prevents ovulation (release of egg from ovary) • Thickens cervical mucus (w/in 24 hrs of insertion)
Nexplanon® • Local anesthetic applied • No incision for insertion • Placed in inner aspect of non-dominant upper arm
Short Insertion and Removal Time Insertion < 1 minute Removal < 3 minutes