Download
1 / 55
1.4k likes | 3.86k Vues
Introduction to Fluoroscopy & Radiation Safety. RTEC 124 - Week 10 Rev 2010. References: Merrills CH 16 & 17 Bushong – Ch 21. CONVENTIONAL FLUOROSCOPY INVENTED BY THOMAS EDISON. Early Fluoroscopy. Digital / Fluoro Equipment Check off. MUST BE COMPLETED PRIOR TO DOING ANY PATIENT EXAMS

E N D
Introduction toFluoroscopy& Radiation Safety RTEC 124 - Week 10 Rev 2010 References: Merrills CH 16 & 17 Bushong – Ch 21
CONVENTIONAL FLUOROSCOPYINVENTED BY THOMAS EDISON Early Fluoroscopy
Digital / Fluoro Equipment Check off • MUST BE COMPLETED PRIOR TO DOING ANY PATIENT EXAMS • Fluoroscopy Procedures must ALWAYS be supervised – even after a check off • You MUST be a CRT to have a Fluoroscopy Lic to operated fluoro units in California (CDPH-RHB Title 17)
Fluoroscopy is a common technique used by clinical physicians to obtain real time images of moving body parts and internal structures of a patient compared to static radiographic examinations. Fluoroscopy: Images in MotionConventional & Digital Fluoro Principles
Objectives • Differentiate fluoroscopic examinations from static diagnostic radiographic examinations • Describe a typical basic fluoroscopic image chain (RT 244 – detailed) • Explain difference between fluoroscopic operation and a diagnostic x-ray tube • Safety Principles
C-arm Under table/over table units Conventional & Digital Units Types of Equipment
Recording the Fluoroscopic Image • Cassettes • 105 mm chip film • Digital fluoroscopy Dynamic Systems • Cine film (cardiac cath) • Videotape (OPMS)
IMAGE INTENSIFICAITONphotons are ampilfied + multiplied • IMAGES ARE VIEWED ON A TV SCREEN/MONITOR
Image Intensifier & Cassette loading Digital & Conventional Units
Image Intensifier Bushong – Ch 21
Conventional Fluoro X-ray tube located under the table
DIGITAL FLUORO X-ray tube located under or over the table – remote controls
Provide Assistance To the Patient And Radiologist Before, during and after the procedure Prep the room Prep the contrast Prep the patient Get a history from the patient Aftercare instructions and clean up of supplies The Role of the Technologist
GI tract studies Esophagus /OPMS Upper GI SMB BE ERCP GU studies - VCU's, RT 255 The “OGRAMS” Angiograms Hysterosalpingograms Venogram Myelogram Sialogram Tube /Line placement Fistulograms ETC ETC PAIN CLINIC (C-ARM) Carlton – Ch. 40Fluoroscopic UsesFunctional studies – xrays in motion
Radiation Safety and Fluoroscopy Time Distance Shielding The Patient & Scatter
Radiation Protection During Fluoroscopy • The patient • The radiographer and radiologist • Others
RADIATION PROTECTIONThe Patient is the largest scattering object • Lower at a 90 DEGREE ANGLE from the patient + PRIMARY BEAM AT 1 METER DISTANCE - • 1/1000 OF INTENSITY PRIMARY XRAY or 0.1%
Room design Remember to move the overhead tube out of the way!
Protective Barriers • Primary barrier – protection from Primary radiation (for the patient& technologist ) • The II is a 2.0 mm pb eq barrier • Secondary barrier - protection from Secondary radiation (from the patient) - Protection for the technologists, etc
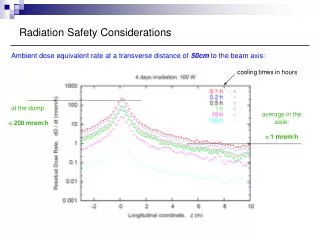
Iso Exposure CurvesWhere is it SAFE?? Behind the lead shield and behind the Radiologist!
Patient entrance skin exposure (ESE) is higher when the fluoroscopic x-ray tube is too close to the tabletop. • Minimum source-to-skin distance • 12” for mobile equipment • 15” for stationary systems • Audible alarm at 5 mins. • Same rules for collimation
PATIENT EXPOSURE KEEP I.I. CLOSE TO PATIENT • REDUCE DISTANCE OF IMAGE INTESIFIER • INCREASE DISTANCE FROM THE TUBE Patient entrance skin exposure (ESE) is ALSO higher when the IMAGE INTENSIFIER is too FAR to from the patient.
Under table tube vs Over table tube (remote units)Digital & Conventional Fluoro
Fluoroscopic X-Ray Tubes • mA range: 0.5 – 5.0 mA • KVP: 70 – 110 • depending on exam and contrast used • 15” minimum SOD in fixed fluoroscopic equipment • Foot switch (dead man)
Fluoroscopic Positioning Previewing • Radiographers are trained in positioning • Unnecessary radiation exposure to patient is unethical • Fluoroscopic equipment should not be used to preview patient’s position
Principles of Personnel Exposure Reduction • Time • Distance • Shielding • Protective barriers • Protective devices
Protection of Radiographer and Radiologist • Lead apron • 0.25 mm Pb/eq • Highest energy scatter • Same level as radiographer /radiologist’s gonads (135o under table) • OR for eyes (over table 45o) see diagrams • 90o angle to the incident beam (lowest) • (without shield – still high • see isoexposure curves)
Used when it is not possible to remain behind a barrier • Lead aprons • Lead gloves • Lead glasses • Thyroid shields • 0.25 –1.0 mm lead eq Protection of Radiographer and Radiologist • Single step away from the table • decreases exposure exponentially (inverse sq law) • Bucky slot cover • Lead rubber drape • Radiologist as shielding
PATIENT – WHEN NOT IN AREA OF INTEREST REMEMBER WHERE THE SOURCE OF THE XRAY BEAM IS COMING FROM! .5MM FOR GONADS TECHNOLOGIST .25 MM LEAD APRON THYROID SHEILD Shielding What is the pb eq? Can this be used for gonads?
Patient Protection • Tabletop exposure rate • Maximum 10 R/min • Typically 1 – 3 R/min • Typical exposure rates • Cinefluorography • 7.2 R/min • Cassettes • 30 mR/exposure • 105 mm film • 10 mR/exposure
ALARA: As Low As Reasonably Achievable • Radiologic personnel are responsible for minimizing radiation exposure to patients • Achieved through thoughtful approach and application of radiation protection practices Procedure dose to patient
Protection of Others • Radiographer’s responsibility to inform others in the room to wear lead apron • Do not initiate fluoroscopy until all persons have complied
Protection of Personnelduring FLUOROSCOPY • Radiologic personnel should not hold patients for exposures • Student SHALL not hold patient during radiation exposure • Family or friend better choice • Immobilization devices best choice
Always make sure the foot Board is correctly in place BEFORE standing a pt on the table Check weight limit for table
BASIC PROCEDURES For FLUOROSCOPY Note – do not allow pt to place Cup on the II - Table will move from vertical to horizontal!
Depending on the study – the patient may begin in the upright position The Radiologist may then place the patient and table recumbant to finish the fluoro study
OVERHEADStaken afterDR leaves room Depending on the study – the patient may begin in the upright position The Radiologist may then place the patient and table recumbant to finish the fluoro study
AFTER FLUOROSCOPY IS COMPLETE LARGER FORMAT IMAGE 14X17 DIGITAL 14X14 MAX “OVERHEADS”