Download
1 / 30
350 likes | 829 Vues
Tocilizumab (RoACTEMRA): a New Therapeutic Approach in Rheumatoid Arthritis. Ronald F van Vollenhoven Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden. Clinical case.

E N D
Tocilizumab (RoACTEMRA): a New Therapeutic Approach in Rheumatoid Arthritis Ronald F van Vollenhoven Rheumatology Unit, Karolinska University Hospital, Stockholm, Sweden
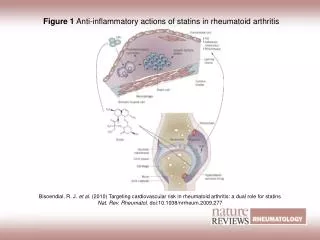
IL-6 is produced by multiple cell types and is associated with numerous biological activities Monocytes/ macrophages Mesenchymal cells, fibroblasts/ synoviocytes Endothelial cells T-cell activation IL-6 Hepatocytes Neutrophils Acute-phase proteins, e.g. hepcidin, CRP Maturation of megakaryocytes B cells Osteoclast activation Bone resorption Hyper--globulinaemia Thrombocytosis Auto-antibodies (RF) Choy E. Rheum Dis Clin N Am 2004;30:405415.Rose-John S, et al. Expert Opin Ther Targets 2007;11:613–624.
Articular effects of IL-6 in RA B cell Antibody production1 Synoviocytes VEGF2 IL-6 Macrophage Endothelial cells Pannus formation3 MMPs4 T cell Neutrophil Joint destruction1 Osteoclast activation, bone resorption Mediation of chronic inflammation5 1Choy E. Rheum Dis Clin North Am 2004;30:405–415.2Nakahara H, et al. Arthritis Rheum 2003;48:15211529.3Yoshizaki K, et al. Springer Semin Immunopathol 1998;20:247259. 4Smolen J, et al. Nat Rev Drug Disc 2003;2:473–488. 5Gabay C. Arthritis Res Ther. 2006;8 (Suppl 2):S3.
Systemic effects of IL-6 in RA Acute-phase response1 Acute-phase proteins (e.g. CRP) IL-6 Hepcidin production Alterations in iron homeostasis2 Thrombocytosis1 Osteoporosis1 Hypothalamus/pituitary/adrenal axis5 Alterations in lipid metabolism3,4 Mood/fatigue/pain6 1Choy E. Rheum Dis Clin North Am 2004;30:405–415. 2McGrath H & Rigby P. Rheumatology 2004;43:1323–1325. 3Al-Khalili L, et al. Mol Endocrinol 2006;20:3364–3375. 4van Hall G, et al. J Clin Endocrinol Metab 2003;88:3005–3010. 5Perlstein R, et al. Endocrinology 1993;132:946952. 6Chrousos G. N Engl J Med 1995;332:1351–1362.
Tocilizumab (RoACTEMRA): anti-IL6 1- Efficacy
37 29 12 Phase III clinical trials with tocilizumab in RA: ACR50 and ACR70 responses MTX-naïve DMARD-IR Anti-TNF-IR p=0.0023 p=0.0002 Tocilizumab 8 mg/kg 44 45 p<0.0001 p<0.0001 Control 40 34 35 p<0.0001 p<0.001 9 30 28 25 Patients (%) 19 20 15 15 10 10 4 5 2 1 0 ACR50 ACR70 ACR50 ACR70 ACR50 ACR70 AMBITION1 RADIATE3 POOLED: LITHE + OPTION + TOWARD2 1Jones G, et al. Ann Rheum Dis 2009 [epub].2Data on file, F. Hoffmann-La Roche pooled analysis: LITHE, OPTION, TOWARD. 3Emery P, et al. Ann Rheum Dis 2008;67:1516–1523.
Phase III clinical trials with tocilizumab in RA: good/moderate EULAR response MTX-naïve DMARD-IR Anti-TNF-IR Tocilizumab8 mg/kg 100 Odds ratio: 4.2 (95% CI 2.9–6.1) p≤0.0001 p<0.0001 Good 82 78 Moderate 80 68 65 Control 40 60 40 Good 17 EULAR response (%) Moderate 37 36 40 5 17 48 42 20 38 2 31 31 15 0 AMBITION1 RADIATE3,4 POOLED: LITHE + OPTION + TOWARD2 1Jones G, et al. Ann Rheum Dis 2009 [epub]. 2Data on file, F. Hoffmann-La Roche pooled analysis: LITHE, OPTION, TOWARD.3Emery P, et al. Ann Rheum Dis 2008;67:1516–1523. 4Data on file, F. Hoffmann-La Roche clinical study report: RADIATE.
Phase III clinical trials with tocilizumab in RA: DAS28 remission (<2.6) MTX-naïve/free DMARD-IR Anti-TNF-IR Tocilizumab 8 mg/kgmonotherapy (n=286) Tocilizumab8 mg/kg + DMARD (n=1,406) Tocilizumab8 mg/kg + MTX (n=170) MTX monotherapy (n=284) Placebo + DMARD (n=1,010) Placebo + MTX (n=158) Odds ratio: 5.8 (95% CI 3.3─10.4) p<0.0001 p=0.0001 40 34 31 30 30 Patients (%) 20 12 10 3 2 0 AMBITION1 POOLED: LITHE + OPTION + TOWARD2 RADIATE3 1Jones G, et al. Ann Rheum Dis 2009 [epub]. 2Data on file, F. Hoffmann-La Roche pooled analysis: LITHE, OPTION, TOWARD.3Emery P, et al. Ann Rheum Dis 2008;67:1516–1523.
Phase III clinical trials with tocilizumab in RA: low disease activity (DAS28<3.2) MTX-naïve DMARD-IR Anti-TNF-IR Tocilizumab 8 mg/kg + MTX (n=170) Tocilizumab 8 mg/kgmonotherapy (n=286) Tocilizumab 8 mg/kg + DMARD (n=1,406) MTX monotherapy (n=284) Placebo + DMARD (n=1,010) Placebo + MTX (n=158) p<0.0001 60 51 50 47 46 40 Patients (%) 30 19 20 10 7 5 0 AMBITION1† POOLED: LITHE + OPTION + TOWARD2 RADIATE2 1Data on file, F. Hoffmann-La Roche clinical study report: AMBITION. 2Data on file, F. Hoffmann-La Roche pooled analysis: LITHE, OPTION, TOWARD.3Emery P, et al. Ann Rheum Dis 2008;67:1516–1523.
= infusions Tocilizumab induces rapid and durable normalisation of CRP • In patients with severe active disease (DAS28 ~6.7) at baseline, tocilizumab normalised CRP in >90% of patients within 2 weeks Placebo + DMARD (n=1,170) MTX (n=284) 3.5 Tocilizumab 8 mg/kg (n=288) 3.0 Tocilizumab 8 mg/kg + DMARD (n=1,582) 2.5 2.0 Mean CRP (mg/dl) 1.5 1.0 0.5 ULN=0.3 0.0 0 2 4 6 8 10 12 14 16 18 20 22 24 Time (weeks) Pooled analysis of AMBITION, OPTION, TOWARD, LITHE and RADIATEULN = upper limit of normal Genovese M, et al. ACR 2008; Poster 987.
Tocilizumab monotherapy vs. MTX: AMBITION trial, ACR responses at 24 weeks MTX-naïve† 100 MTX (n=190) 90 Tocilizumab 8 mg/kg (n=191) p<0.004 80 69 70 60 p=0.01 54 Patients (%) 50 45 p=0.005 40 33 27 30 20 14 10 0 ACR70 ACR20 ACR50 *Post-hoc analysis†Subset of patients never exposed to MTX Jones G et al. Ann Rheum Dis 2009 [epub].
Tocilizumab vs. placebo: radiographic progression at week 52 (LITHE trial) Placebo + MTX (n=393) Tocilizumab 8 mg/kg + MTX (n=398) p<0.0001 1.2 1.1 1.0 p<0.0001 0.8 0.7 p<0.01 0.6 Mean change from baseline 0.4 0.4 0.3 0.2 0.2 0.1 (n=290) (n=348) (n=290) (n=348) (n=290) (n=348) 0 Total Sharp– Genant score Erosion score JSN score Numbers in parentheses are the total numbers of patients who reached the time point and had valid assessmentsJSN = joint space narrowing Kremer J, et al. ACR 2008; Abstract L14.Data on file, F. Hoffmann-La Roche clinical study report: LITHE.
Tocilizumab efficacy • Efficacy demonstrated in various RA populations • TNF-failure, DMARD-failure, MTX-naive • As combination with MTX, as monotherapy • Robust ACR and EULAR responses • Significant proportions of patients achieve LDA or remission • Radiographic efficacy at week 52 (LITHE)
Tocilizumab (RoACTEMRA): anti-IL6 2- Safety
Summary of clinical trials and patients in the all-exposure population TCZ administered once every 4 weeks unless otherwise indicated PBO=placebo; DMARD-IR/TNF-IR=patients with an inadequate response to DMARD/anti-TNF therapy
All-exposure population: Patient retention Cut-off date: 10 March 2008
Tocilizumab exposure during the clinical trial programme (Roche and Chugai) up to 30 June 2008 * Patient-years of exposure are estimated† For Roche, this included a drug-drug interactions study in RA patients (23 patients dosed at 10 mg/kg) ‡Some patients received 4 mg/kg and 8 mg/kg and are accounted for twice in the number for ‘<8’ and ‘≥8’ but only once in the ‘total all doses’ category
Adverse events • Rate of withdrawal attributed to AEs = 6.5/100 PY All-exposure population
Serious infections • Most common infections were pneumonia (n=66) and cellulitis (n=31) • Nine opportunistic infections were reported (0.2/100 PY) • M. avium complex infection, TB (n=2), mycobacterial urinary tract infection, P. jiroveci pneumonia, Candida osteomyelitis, GI candidiasis, fungal oesophagitis and fungal sinusitis All-exposure population
Rates of serious infections • Overall rate of serious infections = 4.37/100 PY (n=249) • Rate of deaths attributed to infections = 0.18/100 PY (n=10) All-exposure population
Overview of M. tuberculosis cases: six reported In all cases, tocilizumab treatment was discontinued TCZ worldwide RA safety database
Patients reporting neutropenia • Clinically significant neutropenia was detected during at least one visit in 156/3,857 (4%) of patients (grade 3, n=139;grade 4, n=17) All-exposure population
Infusion-related events • Overall rate of infusion reactions: • During infusion = 2.8/100 PY • Within 24 hours of infusion = 5.7/100 PY • Clinically significant infusion reactions resulting in treatment discontinuation reported in 15 patients (0.4%) • 8 anaphylactic reactions (0.2%) • 3 infusion-related events (<0.1%) • Hypersensitivity (<0.1%) • Palpitations (<0.1%) • Syncope (<0.1%) • Allergic dermatitis (<0.1%) All-exposure population
Gastrointestinal perforations • Including Roche and Chugai databases (to 30 June 2008): N=5,395; exposure, 9,948 PY • Upper GI tract perforations = 0.6/1,000 PY • Lower GI tract perforations = 1.7/1,000 PY All-exposure population
Cardiovascular events • The most frequent cardiovascular events were arrhythmias and ischaemic events All-exposure population
Malignancies • 81 were confirmed malignancies, 9 were benign neoplasms and 5 were unspecified neoplasms All-exposure population
Percentage of patients with single elevations in transaminase levels ALT AST • 67 (1.7%) patients discontinued treatment because of elevations in transaminase levels • Elevations in transaminase levels were not associated with clinical hepatic events All-exposure population
Tocilizumab safety summary • No new safety signals emerged after prolonged exposure to TCZ • Incidences and types of AEs reported after long-term exposure to TCZ were similar to those reported in controlled 6-month studies • Rates of serious infections, malignancy and other SAEs did not increase with continued treatment with TCZ • With >10,000 patient-years of TCZ exposure, six cases of Mycobacterium tuberculosis infection have been reported • The incidence of elevations in ALT/AST levels did not increase after prolonged administration of TCZ • Elevations in lipid levels were observed with TCZ treatment and decreased when statins were prescribed • Rates of MI/stroke were comparable with those reported for RA patients receiving biologics (<0.5 per 100 PY) and remained stable over time
Final Conclusions • The tocilizumab clinical trials data demonstrate efficacy across RA patient populations and disease outcomes, and a well-defined and manageable safety profile • Together, these findings support a favourable risk/benefit ratio for tocilizumab in patients with rheumatoid arthritis