Download

1 / 42
420 likes | 590 Vues
Insulin sensitizing agents use in pregnancy and as therapy in PCOS. J. SERNA MD. PhD. IVI Madrid. TREAT WHAT?. Imparied. Treatment Options. Weight/Metabolic. Diet/lifestyle Metformin. Dysfunctional bleeding. Cyclic progesterone OCP. Infertility. Metformin Clomiphene Letrozole

E N D
Insulin sensitizing agents use in pregnancy and as therapy in PCOS J. SERNA MD. PhD. IVI Madrid
TREAT WHAT? Imparied Treatment Options Weight/Metabolic Diet/lifestyle Metformin Dysfunctional bleeding Cyclic progesterone OCP Infertility Metformin Clomiphene Letrozole Gonadotropins Ovarian cautery Skin OCP + antiandrogen (spironolactone, flutamide, finasteride) GnRH agonists
Type II anovulatory patients: treatment options • Diet and exercise • Clomiphene citrate, Tamoxiphene • Aromatase Inhibitors • Insulin-Sensitizing Agents • Gonadotropins • FIV-ICSI +/- IVM • Ovarian drilling
TREAT WHAT? Imparied Treatment Options Weight/Metabolic ISA Dysfunctional bleeding ISA Infertility ISA Skin ISA
CLOMIPHENE INDUCTION OF OVULATION IN PCOS • Bad prognostic factors: • BMI >31 • Increased androgens • Amenorrhea • Older patients • Alternatives/associations: • Metformin if IR • hCG • Glucocorticoids • Gonadotropins • Ovarian drilling • Non wanted effects: • Cervical mucus, endometrium ?? • Vascular side effects (11%) visual side effects (2%) • MP 7%, OHSS, SAB ??
Insulin-Sensitizing Agents • α-Glucosidasa Inhibitors • Sulfonilureas • Methiglinides • Biguanides • Thiazolidindiones
Therapeutical Scheme for PCOS Ovulation Aromatase inhibitors?? Drilling???
Ovulation Induction vs. Ovarian Stimulation Ovarian Stimulation Ovulation Induction Women with anovulation Women ovulating Restore oocyte production Increase # oocyte production Monofollicular cycle Polyfollicular cycle
Ovulation and pregnancy OHSS Multiple Pregnancy Anovulation Normal Ovary Polycystic Ovary
Chance of ovulation and of a live birth after CC Imani B. Fertil Steril 2001.
Induces ovulation 6 to 8 folds • Decreases Serum Testosterone • Metformin, but not Rosiglitazone, improves HOMA IS • Rosiglitazone improves ovulation despite no significant improvements in insulin parameters
209 CC 208 Metformin 6 months of treatment 209 CC+Metformin 626 patients 6% 0% 3% CC: 22% Metformin: 7% CC+Metformin:26% Multiple pregnancy Live birth rate: First-trimester pregnancy loss did NOT differ among the groups
CONCLUSIONS: CC is > to metformin in achieving live birth in PCOS, although multiple birth is a complication. No advantage of the combination therapy over the CC Independently of treatment, BMI < 30 had a higher rate of live births Ovulation rate was higher in the combination group
METFORMINA + FSH vs FSH Fedorsäck (2003) • 17 PCOS + IR women 2 cycles with and without metformin • BMI: 32,0 kg/m2 • Metf. do not decreases FSH units needed • Metf. more oocytes were retrieved
METFORMINA + FSH vs FSH SOLO Kjotrod (2004 ) • RCT double-blinded, placebo-controlled • 73 patients random. (BMI><28kg /m2 ): • Placebo/metf. 1000mg /day during 16 weeks
METFORMINA + FSH vs FSH SOLO Kjotrod (2004 ) • Duration of stimulation • Estradiol hCG day • Oocyte number + fertilization rate • Embryo quality • Pregnancy rate SIGNIFICANT DIFFERENCES ONLY IN PCOS BMI< 28 Clinical Pregnancy Rate
Rationale • Is it recommended to continue with metformin during pregnancy? • How long? • Which doses? • Which is the safety profile?
SAB, GD • PCOS patients do have an increased abortion rate • Jakubowicz ------------- 42% • Glueck ------------- 39-73% • Wang ------------- 25% • PCOS patients do have an increased incidence of gestational diabetes • 46% risk
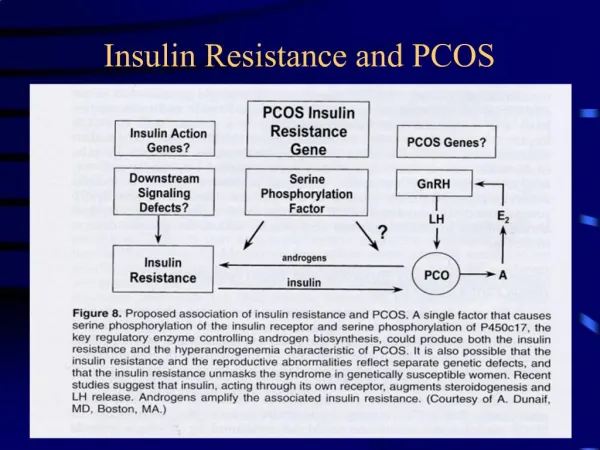
Risk factors: • Hyperinsulinemia, Insulin Resistance • Hyperandrogenemia • Obesity • High PAI-Fas levels inducing hypofibrinolysis • Hyperhomocysteinemia
1st trimester • Jakubowicz et al, JCEM 2002 • Retrospective study in patients with PCOS:
1st trimester • Jakubowicz et al, JCEM 2002 • Retrospective study in patients with PCOS:
1st trimester • Glueck et al: • Decreased SAB rate
Gestational Diabetes • Pregnancy induces a physiologic insulin-resistance increasing insulin needs • PCOS women do have a 46% risk for GD
Gestational Diabetes • Glueck et al: • Decreased GD incidence. Fertil Steril, 2002; Hum Reprod, 2002 Hum Reprod, 2004 • Metformin + diet: • Previous and During Pregnancy Weight Reduction • Weight • [] Insulin, Insulin resistance, Testosterone • Decreased Risk of GD
Safety Profile • FDA group B Either animal-reproduction studies have not shown a fetal risk but there are no controlled studies in women, or animal studies have shown an adverse effect not confirmed by controlled studies in women • Breast-feeding Hale et al, Diabetologia,2002 • Mean doses 1500 mg/day • Mean concentration in babies: 0,28% • < 10%dosage allowed
Small studies non-controlled and short duration Different Bias Most of the obese patients non controlled for hyperinsulinemia Metformin & Pregnancy