The Stroke Continuum
The Stroke Continuum. MA Department of Public Health 2010. CEU’s and CME’s. The Bureau of Infectious Disease Prevention, Response and Services, Massachusetts Department of Public Health, designates this educational activity for a maximum of 1 Credit.

The Stroke Continuum
E N D
Presentation Transcript
The Stroke Continuum MA Department of Public Health 2010
CEU’s and CME’s The Bureau of Infectious Disease Prevention, Response and Services, Massachusetts Department of Public Health, designates this educational activity for a maximum of 1 Credit. Credits will be awarded after successfully completing this slide deck and obtaining at least 80% correct answers on the post- test.
Learning Objectives • Define 2 most common types of stroke. • Identify the stroke continuum. • List 4 modifiable stroke risk factors. • Name 3 observable stroke signs or symptoms. • Describe reason for calling 9-1-1 for stroke signs and symptoms. • Articulate “door-to-needle” goal for tPA administration.
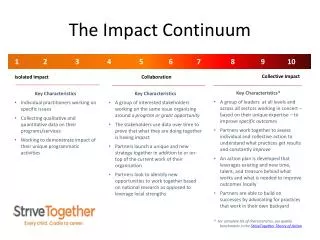
Prevention Re-integration to the Community Recognition Rehabilitation 9-1-1 Inpatient Hospitalization Emergency Medical Services Emergency Department The Stroke Continuum
Stroke: What is it? • Injury or death of brain tissue from oxygen deprivation. • A life threatening emergency.
Blood Supply to the Brain Each artery supplies blood to specific areas of the brain. Stroke occurs when one of these arteries to the brain either is blocked or bursts. Source: National Stroke Association
Temporary blockage <24 hours duration. Symptoms of numbness, trouble speaking, and loss of balance or coordination. Increased risk of having stroke within 90 days. Source: National Stroke Association Transient Ischemic Attacks
Ischemic Stroke • Clot cuts off oxygen to a part of the brain. • Most common stroke (80 – 85% of all strokes).
Embolic A blood clot or plaque fragment that forms in the body moving through the bloodstream to the brain. Thrombotic A blood clot that does not travel but forms inside an artery supplying blood to the brain. Types of Ischemic Strokes
Hemorrhagic Stroke • Burst blood vessel in brain that spills blood into brain tissue. • Accounts for about 15-20% of all strokes.
Types of Hemorrhagic Stroke • Intracerebral hemorrhage: • Blood vessel bursts into the brain • High blood pressure most common cause • Aneurysm: • Weak spot on artery wall that balloons out, forming a thin-walled bubble • Leaks blood into or outside of the brain • Subarachnoid hemorrhage: • Blood vessel bursts near surface of brain pouring blood into area outside brain • Increases pressure on brain
Facts AboutStroke • Stroke can happen at any time, regardless of race, sex or age. • Every 40 seconds someone in the US has a stroke. • Every 3-4 minutes, someone dies from stroke. • Two million brain cells die every minute during stroke, increasing the risk of permanent brain damage, disability or death. National Stroke Association
Facts About Stroke in Massachusetts • In 2007, stroke accounted for 5.1% (2,700) of all deaths and remains the third leading cause of death. MA Vital Records 2007 • In 2007, 2.4% of adults reported having had a stroke. MA BRFSS 2007 • Over 17,000 patients are hospitalized for stroke every year. MA Hospital Discharge Data 2004-2007
Disability • Stroke is a leading cause of adult disability in the US. • With timely treatment, the risk of death and disability from stroke can be lowered. • In 2010, stroke will cost the US $73.7 billion in health care services, medications, and lost productivity. CDC; AHA
Prevention Re-integration to the Community Recognition Rehabilitation 9-1-1 Inpatient Hospitalization Emergency Medical Services Emergency Department The Stroke Continuum
Modifiable Risk Factors for Stroke • High Blood Pressure • Overweight/Obesity • Diabetes • High Cholesterol • Tobacco Exposure • Excessive alcohol consumption • Drug Abuse • Atrial Fibrillation
High Blood Pressure • High blood pressure – higher than 140/90. • Approximately 30% of adults are unaware of their high blood pressure.JNC-7 • More than 40% of individuals with high blood pressure are not on treatment.JNC-7 • 2/3 of people with high blood pressure are not controlled to BP levels <140/90.JNC-7 • 26% of Massachusetts adults have high blood pressure.MA BRFSS 2007
Awareness, Treatment and Control of High Blood Pressure by Age NHANES: 2005-2006. Source NCHS and NHLBI
High Blood Pressure in MA Adults by Age and Gender MA BRFSS 2005, 2007
High Blood Pressure in MA Adults by Race, Ethnicity and Gender MA BRFSS 2003,2005, 2007
Overweight and Obesityin Massachusetts • 56.1% of adults are overweight or obese. • 22% of adults are obese. • 73% do not eat the recommended. five or more servings of vegetables and fruits a day. • 49% do not get regular physical activity. MA BRFSS 2007
Obesity Trends Among U.S. Adults, 1995 No Data <10% 10%–14% 15%–19%
Obesity Trends Among U.S. Adults, 2000 No Data <10% 10%–14% 15%–19% ≥20%
Obesity Trends Among U.S Adults, 2005 No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
Diabetes • In Massachusetts, 7.4% of adults have been diagnosed with diabetes.MA BRFSS 2007 • CDC estimates that an additional 2.2% of Massachusetts adults don’t know that they have diabetes. • People with diabetes are two to four times more likely to have a stroke.National Stroke Association
Overweight and Obesity in US Children and Adolescents NHANES, 1971-74, 1976-80, 1988-94 and 2001-2004). Source: Health, United States, 2006, NCHS.
High Cholesterol in MA • 35.6% of MA adults have high cholesterol. MA BRFSS 2001-2007 • The prevalence of high cholesterol has been increasing each year. MA BRFSS 2001-2007 • Low HDL cholesterol (the “good” kind) in men is a risk factor for stroke. American Stroke Association
Tobacco • Cigarette smoking approximately doubles a person’s risk for stroke. CDC • In MA, the cities of Springfield, Fall River, New Bedford, Lowell, and Worcester have significantly higher rates of smoking than MA overall. MA BRFSS 2007
Excessive Alcohol Consumption • Chronic, excessive alcohol intake can precipitate hemorrhagic stroke: • No more than 2 drinks per day for men and no more than 1 drink per day for non-pregnant women. AHA • Most risk from excess alcohol intake is likely due to high blood pressure and impaired blood clotting mechanisms. National Stroke Association
Drug Abuse • Use ofcocaine, amphetamines, and heroin associated with an increased risk of stroke. • Strokes caused by drug abuse are often seen in a younger population. American Heart Association
Atrial Fibrillation • Characterized by an irregular and frequently fast heartbeat, atrial fibrillation (AFib) is the most common form of heart arrhythmia. • Associated with a five-fold increase in risk for stroke. • About 15% of people with strokes have Afib. • Increases the risk of death from stroke. National Stroke Association
Prevention Re-integration to the Community Recognition Rehabilitation 9-1-1 Inpatient Hospitalization Emergency Medical Services Emergency Department The Stroke Continuum
Signs and Symptoms • Only 23.3% of Massachusetts adults recognize all stroke signs and symptoms. MA BRFSS 2007
Stroke Heroes Act FAST • Educational kit for Train the Trainer Model. • Media campaign – TV, radio, newspaper and transit ads. • Cultural adaptation – English, Spanish, Portuguese, and Khmer.
Stroke Heroes Act FAST • ADD ANIMATION HERE
F = Face • Droops on left or right side • Sudden drooling • Numbness Ask person to smile
A = Arms • Look for difficulty holding things or putting on clothing • Numbness • One arm drifts down or won’t go up • May have trouble walking Ask person to raise both arms
S = Speech • Slurred speech • Doesn’t make sense • May not understand what other people are saying • Forgets how toread or write Ask to repeat phrase or name object
T = Time • Time lost is brain lost • Save time and brain cells, go in an ambulance At any sign, Call 9-1-1
The “Suddens” • Sudden numbness or weakness of face, arm, or leg, especially on one side. • Sudden confusion, trouble speaking or understanding speech. • Sudden trouble seeing in one or both eyes. • Sudden trouble walking, dizziness, loss of balance or coordination. • Sudden severe headache with no known cause.
Prevention Re-integration to the Community Recognition Rehabilitation 9-1-1 Inpatient Hospitalization Emergency Medical Services Emergency Department The Stroke Continuum
Time Lost = Brain Lost Delays in calling 9-1-1: • Most strokes are painless. • Symptoms can be subtle. • Person having a stroke may be unaware or unable to communicate. • Observers do not recognize it as a serious problem.
EMS Care is Critical • Identification of stroke by conducting stroke scale assessment. • Establish “last known well” time. • Pre-notification to hospital to activate stroke team. • Transport to most appropriate hospital for stroke care.
Prevention Re-integration to the Community Recognition Rehabilitation 9-1-1 Inpatient Hospitalization Emergency Medical Services Emergency Department The Stroke Continuum
Primary Stroke Service (PSS) in MA • MDPH regulations passed by the state legislature in 2004. • Assure ambulances take patients to hospitals that can provide definitive care. • Improve coordination of care/pre-hospital care for persons experiencing stroke symptoms. • Assure hospitals have systems in place to accurately diagnose and treat, 24 hours per day, 7 days per week.
Primary Stroke Service (PSS) in MA • Assure data available to monitor system performance. • Emergency diagnostic and therapeutic services provided by a multidisciplinary team. • Time targets: • Door-to-stroke team: 15 minutes • Door-to-CT scan: 25 minutes • Door-to-needle: 60 minutes
Stroke Treatment Activase® (alteplase, recombinant, IV-tPA, tPA), was approved by the FDA for the treatment of acute ischemic stroke. • IV-tPA isrecommended for selected patients within 3 hoursof “last known well”. (Class I, LOE A) • IV-tPA should be administered to eligible patients within 3.0-4.5 hours of “last known well”. (Class I Recommendation, LOE B) Adams, Stroke 2007
Meta-Analysis of the major IV tPA trials shows clear benefit up to 3 hrs and NOW beyond NINDS 12% ECASS3 7% Lancet, 2004; 363: 768–74