Download
1 / 26
270 likes | 290 Vues
Learn about U.S. FDA's role in ensuring TMD medical product safety and efficacy, including device classification, mouthguards, dental materials, TMJ implants, postmarket assessment, and surveillance studies.

E N D
US Regulation of TMD Medical Products Malvina B. Eydelman, M.D Director Division of Ophthalmic, and Ear, Nose, and Throat (ENT) Devices Acting Director Pilot Office of Ophthalmic, Dental, Respiratory, Anesthesia, and ENT Devices Center of Devices and Radiological Health U.S. Food and Drug Administration
FDA Mission • The Food and Drug Administration is responsible for protecting the public health by ensuring the safety, efficacy, and security of human and veterinary drugs, biological products, and medical devices; and by ensuring the safety of our nation's food supply, cosmetics, and products that emit radiation. • FDA also has responsibility for regulating the manufacturing, marketing, and distribution of tobacco products to protect the public health and to reduce tobacco use by minors. • FDA is responsible for advancing the public health by helping to speed innovations that make medical products more effective, safer, and more affordable and by helping the public get the accurate, science-based information they need to use medical products and foods to maintain and improve their health. • FDA also plays a significant role in the Nation's counterterrorism capability. FDA fulfills this responsibility by ensuring the security of the food supply and by fostering development of medical products to respond to deliberate and naturally emerging public health threats.
Medical Products • Biological Product • Drug • Device • Combination Product
Center for Devices and Radiological Health (CDRH) Regulates All Medical Devices
Office Director – Malvina B. Eydelman, M.D. Deputy Director Associate Director Deputy Director Associate Director for Operations Chief Medical Officer Associate Director for Professional Development (PD) Office Staff Assistant Director for PD Safety Signal Manager Division of ENT, Sleep, Respiratory, and Anesthesia Devices Division of Dental Devices • Division of Ophthalmic Devices Intraocular Lenses and Accessory Devices Implantable Dental Devices Anesthesia Devices OFFICE OF OPHTHALMIC, DENTAL, ENT, SLEEP, RESPIRATORY AND ANESTHESIA DEVICES Ear, Nose, and Throat Devices Contact Lenses and Dry Eye Devices Restorative and Surgical Dental Devices Respiratory Devices Retinal and Diagnostic Devices Sleep Disorder Breathing Devices Glaucoma, Cornea, and Surgical Devices TPLC Pilot
Medical Device1 • Definition • Intended to diagnose, cure, mitigate, treat or prevent a disease/condition, or • Intended to affect the structure or function of the body, and • Does not achieve intended use through chemical action or metabolism 1Sec. 201, Food, Drug and Cosmetic Act
Device Classification1 • CLASS I • Simple design, low risk • General Controls • Most exempt from premarket submission • CLASS II • More complex, moderate risk • General Controls plus Special Controls • Premarket Notification [510(k)] • Demonstration of substantial equivalence • CLASS III • Most complex, highest risk • General Controls and Premarket Approval (PMA) • Reasonable assurance of safety and effectiveness 1http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/Overview/ClassifyYourDevice/
MOUTHGUARDS • Class II (recommended) • Over the Counter (Procode OBR, OCO) • Prescription (Procode MQC, OCO) • ~70 510k clearances • 2018 – most recent • Indications • to protect the teeth from damage caused by bruxism, clenching and severe muscle contraction, migraine, TMD or TMJ syndrome (treatment / pain reduction)
Dental Materials • Class II • Prescription (Procode EBI) • ~ 280 510k clearances • Indications • for fabrication of occlusal splints or night guards • Utilized by Dental labs to fabricate mouthguards and splints unique to individual patient • At Direction of Dentist
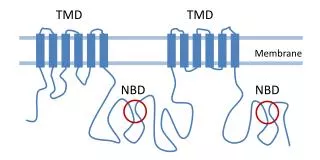
TMJ Implants • Class III – 4 PMAs • Reclassification and Call for PMAs (1998) • P980052 - TMJ Concepts Total TMJ Prosthesis (LZD) • P000023 - The TMJ Implants, Inc. TMJ Fossa-Eminence/Condylar Prosthesis System (now Nexus) (LZD) • P000035 - TMJ Implants, Inc. TMJ Fossa-Eminence Prosthesis (now Nexus) (MPI) • P020016 - Biomet Microfixation/Walter Lorenz Total Temporomandibular Joint Replacement System (LZD)
Postmarket Assessment of TMJ Implants - 2011 • MDRs received by the FDA, indicated many implanted TMJ devices were removed (explanted) in less than three years • Post-approval studies for TMJ implant devices did not adequately address the timing or reasons for device replacement • FDA concluded adequate data to determine the natural lifecycle of implanted TMJ devices had not yet been obtained
522 Postmarket Surveillance Studies Class II or III devices that meet any of the statutory criteria https://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/PostmarketRequirements/PostmarketSurveillance/ucm134497.htm
Section 522 Postmarket Surveillance Orders • Postmarket Surveillance Orders issued on February 4, 2011 to address the following questions: • At what time interval (in months) after initial implant do revisions occur? What is the survival rate for each year post initial implant? What are the mean and median times to failure? • How does patient diagnosis leading to initial device placement impact the timeframe to revision? • At what time interval (in months) after initial revision does any subsequent revision occur? What is the survival rate for each year post-initial revision? What are the mean and median times to failure? • Among initial revisions, what are the reasons for revision? Among patients who have had one previous revision, what are the reasons for a second revision? Among patients with more than one revision, what are the reasons for the subsequent revisions? • What are the modes and causes of failure based on analysis of all of your reasonably available explanted retrieved devices? What is the association between the patients’ demographic and clinical data and device failure? • What is the time to revision among patients with an initial partial implant? In each year after the initial implant, what proportion of patients with a partial implant requires revision with a total TMJ device? • Issued to Biomet Microfixation, TMJ Concepts, and Nexus CMF
Current Status of Section 522 Postmarket Surveillance Orders
The Accelerating Pace of Change: Information Age and Digital Revolution
Partner with Stakeholders to Expedite Innovation Industry Researchers Professional Societies Medical Device Ecosystem Venture Capitalists Regulators Patients Payers Health Care Providers
Statement of Task • Review and estimate the public health significance of TMDs, including prevalence, incidence, burden and costs; and review challenges to data collection and reliability. • Evaluate the evidence base for assessment, diagnosis, treatment, and management of acute and chronic TMD. Recognizing that TMDs are diverse and multifactorial conditions influenced by genetics, sex and gender, environmental, physiological, and psychological factors, this effort will: • Address patient heterogeneity and challenges to patient stratification to better target therapies toward patients. • Identify similarities and differences between chronic TMD, other chronic pain states (as well as chronic overlapping pain conditions), and other joint disorders such as phenotypic features that might predict responsiveness to treatments. • Identify and characterize other non-pain comorbidities that diminish quality of life, including those that affect etiology and influence resilience, such as nutritional challenges and other neurological, metabolic, and mental health conditions (e.g. anxiety, depression). • Examine the evidence-base for defining chronic TMD as a multi-system disorder that necessitates multidisciplinary research and interventions.
Statement of Task (continued) • Identify barriers to appropriate patient-centered TMD care, in the presence and absence of an evidence base, and strategies to reduce these barriers along the continuum of TMD pain. This effort will: • Evaluate elements and outcomes of patient-centered TMD care. • Identify challenges to dissemination and implementation of evidence-based treatments and prevention strategies that are safe and effective. • Determine and characterize health inequities in clinical TMD management. • Review the state of science for TMD and provide an overview of basic, translational, and clinical research for TMD. This effort will: • Examine existing or emerging TMD animal models and their preclinical utility. • Identify gaps and opportunities in TMD research relating to central and peripheral mechanisms, genetic/epigenetic contributions, heterogeneity of molecular mechanisms, joint mechanics, neuroimmune processes, endocrine influences, role of the microbiome, and endogenous mechanisms of resilience. • Assess the intersection of sex differences in immune/neuroimmune and inflammatory responses in chronic TMD with other autoimmune diseases that are more prevalent in females or males.
Statement of Task (continued) • Assess progress on identification and validation of targets and biomarkers (genetic, neuroinflammation, neuroimaging, proteomic, behavioral, etc.) for use in establishing risk, diagnoses, treatment, outcomes, and reoccurrence. • Identify potential approaches to using artificial intelligence for pattern recognition in patient datasets (e.g., genetic, biological, psychological, social traits, electronic health records, and patient-reported outcomes) to distinguish disease subtypes, develop individualized clinical decision support, and predict patient responses. • Identify new and rapidly evolving tools and technologies with potential to significantly advance research, diagnosis, and treatment of TMD. • Identify opportunities and challenges for development, dissemination, and clinical implementation of safe and effective clinical treatments for TMD, including pharmacological agents, regenerative medicine, behavioral interventions, and complementary and integrative approaches. • Identify scientific and clinical disciplines needed to advance TMD science and the development, dissemination, and implementation of safe and effective treatments; as well as strategies to enhance education and training in these disciplines. • Identify multidisciplinary/interdisciplinary research approaches necessary in the short-and long- term to advance basic, translational, and clinical TMD research and to improve the assessment, diagnosis, treatment, and management of TMDs.
Where can patient input inform medical device development and evaluation? Patient-Informed Needs Patient-Centered Outcomes Patient Preference Benefit-Risk Information Patient-Informed Clinical Trial Design, Patient Reported Outcomes Communicating Benefit-Risk Information to Patients