Download

1 / 22
730 likes | 2.38k Vues
Introduction to AFP Surveillance. Polio Eradication Strategies. 1. High routine immunization coverage 2. National Immunization Days (NIDs) 3. Acute Flaccid Paralysis (AFP) surveillance 4. ‘Mop-up’ campaigns. Polio Eradication.

E N D
Polio Eradication Strategies 1. High routine immunization coverage 2. National Immunization Days (NIDs) 3. Acute Flaccid Paralysis (AFP) surveillance 4. ‘Mop-up’ campaigns Polio Eradication
Objectives and main strategy of AFP surveillance for Polio Eradication 1) Objectives: - detect polioviruses wherever they should still circulate -> to target immunization campaigns / mop-ups - show the absence of wild polioviruses - show that surveillance meets the level needed for certification. 2) Strategy: - report and investigate all cases of acute flaccid paralysis - collect and analyze stool specimens to identify polioviruses
How to 'prove' that polio is eradicated? How can we be certain that there is no wild poliovirus in a country that reports “0” cases of polio?
Several other diseases look like clinical polio – true polio cases may be mis-diagnosed (Guillain-Barré Syndrome) reporting of 'clinical polio' is not sensitive – likely to miss cases Increase sensitivity to detect remaining polio by reporting a syndrome – Acute Flaccid Paralysis – which should include all polio cases immediate reporting of all AFP in children < 15 yrs separate true polio from non-polio AFP through testing of stool specimens for wild poliovirus Why report 'AFP' and not 'Polio'?
Steps of AFP surveillance AFP surveillance is the gold standard for detecting cases of poliomyelitis. The FOUR STEPS of surveillance are: • Finding and reporting children with acute flaccid paralysis (AFP) • Transporting stool samples for analysis • Isolating and identifying poliovirus in the laboratory • Mapping the virus to determine the origin of the virus strain.
Acute Flaccid Paralysis Acute:rapid progression of paralysis, (from onset to maximum paralysis) Flaccid:loss of muscle tone, “floppy” (as opposed to spastic or rigid) Paralysis:paresis, weakness, loss or diminutionof motion
Standard Case Definition Acute Flaccid Paralysis (AFP) Any patient under 15 years of age with acute flaccid paralysis, or a patient of any age in whom a clinician suspects polio
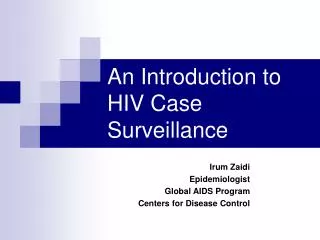
transverse myelitis Other enteroviruses traumatic neuritis Acute flaccid paralysis Coxsackie virus Echovirus Guillain-Barre Syndrome Poliovirus
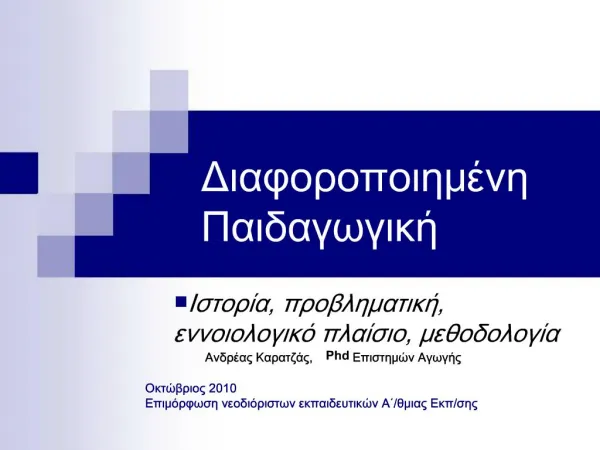
AFP Surveillance System AFP Cases Hospitals Clinics Community Case Investigation and lab analysis Polio AFP Non- Polio AFP Non- Polio AFP rate should be > 2/100,000 <15 years
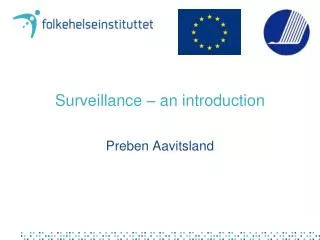
The Process Onset of paralysis Detection & notification Primary culture results reported to EPI < 28 days of specimen receipt < 14 days of onset < 3 days of being sent Case investigation & specimen collection Specimens arrive at national lab Isolates sent to regional lab for intra-typic differentiation > 60 days of onset Intra-typic differentiation results reported to EPI < 28 days of isolate receipt Follow-up exam Classification of case (< 90 days of onset)
All countries have systems for 'routine' (monthly) reporting of selected notifiable diseases (from < 10 to > 50 conditions) health center – district – national level 'passive reporting', often part of overall health management information systems Main problems: not timely, incomplete, data not used to take action Weekly 'zero-reporting' to improve timeliness and completeness: All health facilities should be vigilant for AFP - submit weekly written report on AFP, even if no case was seen IMMEDIATE NOTIFICATION OF AFP CASES, followed by case investigation, stool collection + processing, follow-up exam Routine 'zero-reporting' of AFP
Quality of Acute Flaccid Paralysis (AFP) surveillance Irrespective of poliovirus circulation: at least 2 AFP cases per 100,000 population under 15 years of age 'Sensitive' surveillance for polio: AFP case detection rates of >2 per 100,000 children very likely to detect poliovirus if present AFP case investigation and stool collection: Case investigation, and collection of 2 stool specimens, within 2 weeks of paralysis
Two key indicators to measure performance of AFP surveillance Non-polio AFP rate (NPAFP) - Minimum 'operational' target: ≥ 2/100,000 population <15 yrs • Indicator for 'sensitivity': if NPAFP is > 2/100,000, likelihood of missing true polio cases is very low % AFP cases with 'adequate' specimens - Minimum target: ≥80% of all AFP with adequate stools • Reliable laboratory results are key for good surveillance • "Adequate": 2 specimens collected 24 hours apart within 14 days after onset of paralysis, arriving at the lab in good condition
Stool sample collection procedures for AFP case
Indication for stool collection To identify presence or absence of Polio virus in the stool specimens
Outline • Stool collection • Materials for collection • Procedure of stool collection • Storage, transportation and reversed cold chain • Challenges
AFP Stool collection • Issues to consider for stool collection • Ensure the child fulfil the criteria of true AFP case • Age: <15years or clinician suspect polio • Paralysis: FLACCID/FLOPPY, not spastic • Onset of paralysis: should be < 60 days (If >60 days, Just complete CIF and follow-up exam)
Procedure of stool collection • 2 Stool specimens • Two specimens should be collected at least 24-48 hours apart • Best time to collect samples within 14days of onset of paralysis but sample can collect up to 60days of onset of paralysis • Each sample should be adequate (8gm) in amount
Condition of Stool Specimen Upon arrival at laboratory, stool specimen should show: • No desiccation (not dried-out) • No leakage • Adequate documentation • Evidence that the cold chain was maintained
Further Instructions: If the patient cannot produce stool, leave the collection kit, specimen carrier box and frozen ice packs in the health facility or with the family Explain in simple language the specimen collection procedure. Return at a later time to collect the specimen container box Transportation arrangements should have been made in advance to transport the stool specimens as soon as possible to the laboratory (this is the reverse cold chain system).