Download
1 / 55
660 likes | 1.68k Vues
Chapter 1 Developmental disturbances of teeth Chapter 2 Dental caries Chapter 3 DISEASES OF THE PULP & PERIOAPICAL TISSUES. Etiological factors of pulp diseases : - Most changes in the pulp are caused by irritation. -The main irritants to the pulp belong to two groups :

E N D
Chapter 1 Developmental disturbances of teeth Chapter 2 Dental caries Chapter 3 DISEASES OF THE PULP & PERIOAPICAL TISSUES
Etiological factors of pulp diseases : - Most changes in the pulp are caused by irritation. -The main irritants to the pulp belong to two groups : Group I : living irritants (microbial ) Group II : non-living irritants (non-microbial ) 1) physical : mechanical , thermal , electrical , aeronautical & irradiation. 2) chemical : acids , alkalies & poisons. I- living irritants (microbial irritation ) The principal pathways by which microorganisms may gain enterance into the pulp or periodontal areas are : a) through an open cavity that may be caused by trauma , operative dental procedures or dental caries. b) Via the gingival cervice & by invasion along the periodontal ligament in several forms of periodontal disease. c) By extension of periapical infection from adjacent infected teeth. d) Through the blood stream during bacteraemia or septicemia ( hematogenous infection)
II- Non-living irritants ( non-microbial irritation) A)Mechanical irritaion such : 1- Accidental 2- Odontoiatrogenic ( dentist induced pulpitis). B) Thermal irritation such as : 1- odontogenic 2- large metallic filling without an efficient lining . 3- prologed cooling of teeth. 4- rapid olishing of teeth or restorations. 5- prolonged contact of thermal pulp testers , whether hot or cold . 6- using of Laser for tissue ablation. C) Electrical irritation : When metal fillings of different electromotive potential (gold vs amalgam) are placed so that they occasionally come in contact with each other , an intermittent electrical current may be set up which is of sufficient intensity to irritate the pulp. D) Aeronautical irritation : - Aeronautical odontalgia (Aerodontalgia) denoting toothach occuring to persons of air crews when flying at high altitudes or when entering the low pressure chamber
-This condition may occur in a vital pulp with caries or a filling . -This pain has been attributed to the formation of nitrogen bubbles in the pulp tissues or vessels. It may due to fat emboli from altered lipoprotein & platelet thrombi. -Aerodontalgia is a marker of inadequate pulp protection from the atmosphere & this usually means caries. -So it is not a direct cause of pulpitis , rather than an exacerbation factor. -This condition is also seen in divers subjected to rapid decomposition following deep sea diving. 2) Chemical irritation : Irritant substances may be applied directly to an exposed pulp or may diffuse through the dentine after the insertion of a restorative material.
DISEASES OF THE PULP Classification of pulp disease : Pulp disease of an inflammatory origin can be classified according to : The type of inflammation : A) Focal reversible pulpitis. B) Acute pulpitis C) Chronic pulpitis
Focal reversible pulpitis: ( pulp hyperemia ) A tooth with F.R.P. is sensitive to thermal changes .It is regarded as a reversible condition provided the irritant is removed before the pulp is severely damaged Clinical features : A tooth with F.R.P. is sensitive to thermal changes , particularly cold . Pain disappears upon removal of the stimulus or resolution of normal temperature. Teeth wit F.R.P. usually show deep carious lesion , large metallic restorations without adequate isolation , or restorations with defective margins. Histological features : This is characterized histological by : 1- Dilatation of the pulp vessels. 2- Inflammatory fluid exudate may collect due to the increased passage of tissue fluid through the distended vessels. 3- The escape of the fluid exudate may lead to haemoconcentration & this will lead to increased viscosity of the blood , which thus circulates at a slower rate.
Clinically- • Irreversible pulpitis – Responds to pulp testing – Actively resorbing Possibly non-responsive to pulp testing
B) Acute pulpitis : Definition : -Acute inflammation of the pulp rapidly follows hyperemia if the invading organisms are sufficiently virulent or the resistance is lowered. It may also occur as an acute exacerbation of a chronic inflammatory process. -The first reaction starts when the carious process reaches the junction between enamel & dentine . It is mainly limited to the part of the pulp directly below carious dentinal tubules ( partial acute pulpitis). -The appearance of pulpitis is that of non-specific inflammation . It is a dynamic process. The irritant must reach certain strength before it causes pulp inflammation . -Since pulpitis in most cases is due to a carious lesion , this variant will be described as representative of most cases of pulpitis. The mechanism of pulpitis due to caries is to some extent different from that attributable to other causes but the result is the same . Mechanism of formation of acute closed pulpitis.: -The first reaction starts when the carious process reaches the junction between enamel & dentine. It is mainly limited to the part of the pulp directly below the carious dentinal tubules :
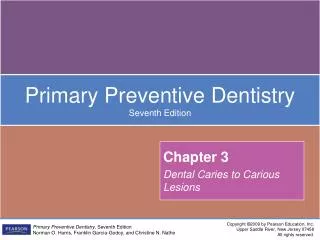
Pulpal hyperaemia. While bacteria are still some distance from the pulp, acid permeating along the dentinal tubules gives rise to hyperaemia, oedema and a light cellular inflammatory infiltrate in the pulp. Cracked tooth. The pulp died beneath this crack which was undetected clinically but which has opened up after decalcification of the tooth.
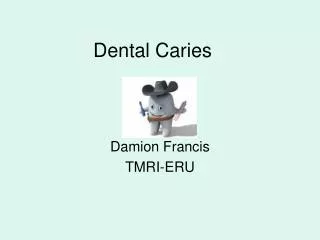
Acute pulpitis. Infection has penetrated the reactionary dentine causing inflammation to spread down the pulp and pus to form in the corner. Acute pulpitis. Beneath the carious exposure (top right) a dense inflammatory infiltrate is accumulating. More deeply, the pulp is intensely hyperaemic.
Acute pulpitis. Infection has penetrated the reactionary dentine causing inflammation to spread down the pulp and pus to form in the corner. Acute pulpitis - terminal stage. The entire pulp has been destroyed and replaced by inflammatory cells and dilated vessels.
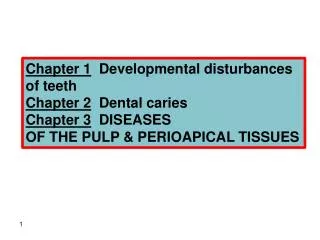
Acute caries and pulpitis. Infection has penetrated to the pulp. Part of the pulp has been destroyed, and an abscess has formed, containing a bead of pus.
1- vascular dilatation . 2- Swelling of odnotoblastic nuclei due to osmotic imbalance. 3- Complete destruction of odontoblasts. 4- Abscess formation . 5- Thrombosis of blood inside the blood vessels may occur due to : a- accumulation of the inflammatory exudate (I.F.E.) increases the pressure outside the vessels. b- Slowing of the blood flow & haemoconcentration of the blood inside the pulp vessels may occur with subsequent death of the pulp. 6- Pulp necrosis Clinical features : 1) is characterized by pain , severe continuous throbbing type. The severity of pain increases while the patient is lying down & with change in temperature . The extreme pain is due to the fact that in pulp inflammation , edema is confined in a rigid chamber of dentine & the pressure is greater that that in loose C.T. This pressure , as wall as the products of inflammation such histamine & serotonin , ac upon the nerve endings to produce pain
Microscopic appearance : - Abscess formation is most likely to occur when the enterance to the pulp is minute & drainage is inadequte . In this stage the number of PMN leukocytes increases & great collections of leukocytes will be found just beneath the area of carious penetration or deeper within the pulp tissue. - A great number of leukocytes become necrotic & die releasing proteolytic enzymes which dissolve the pulp tissue resulting in liquefaction necrosis & the production of pus. This way an abscess is formed which contains inflammatory cells , microorganisms , & tissue debris. The first abscess is most commonly seen in pulp horn. - Adjacent to & surrounding the abscess there is an area containing a dense mass of lymphocytes , plasma cells & monocytes. Microorganisms are present only within the abscess & the nearest layer , associated with necrotic cells. Near the mass of the cells there is deposition of collagen acting as a local protective layer walling off the infectious material or the content of the abscess. If the process has been enclosed within a collagen wall , this can calcify & complete the isolation of the necrotic tissue.
- Further towards the normal pulp there are dilated vessels . Abscesses can be formed in different parts of the pulp at the same time but evatually the whole pulp is transformed into a dead mass of tissue. In this case the suppurative exudate is not localized , & entire pulp is involved. This condition is described as total suppurative pulpitis. 2) With electric tester tooth reacts at a far lower threshold than normal. Treatment consists of : 1- Removal of the cause . 2- Root canal treatment.
Chronic pulpitis : Chronic pulpitis follows injuries similar to those leading to acute pulpitis . The etiology is the same as that of acute pulpitis except that the irritant is of low virulence & therefore the response is milder. Causes : 1- May develop as a sequel of acute pulpitis. 2- When the irritant is not severe enough to cause acute infections i.e. a- when organisms are of low virulence. b- When caries is progressively slowly. 3- When the pulp is capped following traumatic exposure. 4- When caries is not completely removed from a cavity. 5- It may develop in normal teeth not affected by caries , through haematogenous infection ( Anachorectic pulpitis) . Clinical features : 1- The tooth may exhibit intermittent dull aching pain. 2- Sensitivity to heat & cold id less that that in acute pulpitis due to degeneration of nerve fibers. 3- The tooth responds at a higher level to electric pulp tester than does the normal
A Chronic pulpitis. A. Another pulpitis and formation of a calcific barrier. B. This higher power view shows the calcific barrier in more detail, in particular its irregular structure and failure to hold back the infection. B
Mechanism of formation & microscopic findings: 1) Bacterial toxins found in the carious cavity reach the pulp via lymph , which circulates in the dentinal tubules. 2) The toxins are not strong enough to destroy the odontoblasts , but are sufficiently irritating to odontoblastic processes. 3) Odontoblasts rapidly lay down new dentine . The newly formed dentine may be termed secondary or reparative dentine. 4) The involved tubules are sealed off by a hyaline layer or calcified material & more or less irregular secondary dentine is laid down. 5) this tends to reduce the access of irritants to the pulp , & it is probable that the inflammation will resolve more or less completely. 6) Small numbers of bacterial enter the pulp ; they are called “ pioneer microorganisms “. 7) If the defense process continues with sufficient speed & the advance of the carious process is slow , the degree of inflammation may remain mild & is hardly recognizable . 8) When qualitative & quantitative change in the bacteria occurs , the picture may be changes by :
A) Introduction of leukocytes in large numbers , chiefly lymphocytes & plasma cells. B) Formation of small abscess may occur. 9) Capillaries are usually prominent , fibroblastic activity is evident & collagen fibers are seen often gathered in bundles. This is an attempt by the pulp to wall off the infected area from the remainder of it is tissue through deposition of collagen fibers about the inflammed area. Treatment : The same as of acute pulpitis .Either root canal treatment or extraction. Classification : Chronic pulpitis classified into : 1- Chronic closed pulpitis. 2- Chronic opened pulpitis i)Chronic open ulcerative pulpitis. ii) Chronic open hyperplastic pulpitis ( pulp polyp . I) Chronic open ulcerative pulpitis: Here the entire pulp or the greater part of it is shows chronic inflammatory changes. In the area of carious exposure the pulp tissue is replaced by granulation tissue infiltrated with lymphocytes , macrophages & other chronic inflammatory cells.
Open pulpitis. Beneath the wide exposure the pulp has survived in the form of granulation tissue with the most dense inflammatory infiltrate beneath the open surface. Pulp capping. The procedure has allowed the pulp to survive until reactionary dentine has proliferated greatly beside the exposure. Failure of the procedure is indicated by the inflammatory cells concentrated below the opening
Pulp polyp. A hyperplastic nodule of tissue is growing out through a wide exposure of the pulp. The masses of inflammatory cells and the many new vessels are characteristic of granulation tissue. Pulp polyp. An inflamed nodule of granulation tissue can be seen growing from the pulp chamber of this broken down first permanent molar.
Pulp polyp. In this broken down molar, granulation tissue is proliferating from the pulp cavity and has acquired an epithelial covering over much of its surface. Note also the internal resorption (left) as a result of pulpal inflammation. Pulp stones. A rounded nodule of calcified tissue in which some irregular tubules may be seen is present in the pulp. Smaller stones and amorphous calcifications surround the main mass (trichrome stain).
Pulp polyp involving the permanent second mandibular molar in a young adult with multiple carious teeth. Pulp polyps involving the primary, first, and second mandibular molars in a young child with extensive dental caries
Low-power photomicrograph of a pulp polyp demonstrating inflamed fibrovascular tissue that is lined by stratified squamous epithelium (hematoxylin and eosin, original magnification X40). Fibrosed pyogenic granuloma of the mandibular gingiva that partially surrounds a carious molar with crown destruction. Reactive gingival lesions that extend into a large carious lesion of an adjacent tooth may resemble a pulp polyp. Intermediate-power photomicrograph of a pulp polyp with superficial bacteria and exogenous, pigmented material overlying the surface epithelium (hematoxylin and eosin, original magnification X100).
Edema in the pulp escapes from the superficial part of the tissue through the exposure. Symptoms range from none to a minimum , with slight irregular pain of a dull character made worse by thermal changes. II – Chronic open hyperplastic pulpitis: This form of chronic pulpitis occurs either as chronic form from onset or as a chronic stage of a previously acute pulpitis. It occurs particularly in deciduous molars in which extensive carious lesions lead to wide exposure of the pulp . Clinical features : The clinical features of chronic open hyperplastic pulpitis ( pulp poly) are as follows : 1- It appears as a globular mass of tissue protruding from the pulp chamber & often filling the entire cavity. It is usually seen in teeth of children & young adults , with large apical foramina & excellent blood supply , mostly involving the deciduous molars & first permanent molars. 3- When the polyp is young , it bleeds easily ; later on , no bleeding. 4- With age , the structure may become pedunculated , lobulated , & assume the characteristics grossly & microscopically , of the gingiva. 5- Gradually the surface becomes epithelized as a result of implantation of
Of desquamated epithelial cells on it is surface . These grow on the raw pulp surface until it becomes covered by a well formed layer of epithelium . This covering helps protect the nodule of pulp from infection. Inflammation dies down & the granulation tissue changes into collagenous fibrous tissue. 6- On palpation with a probe , slightly sensitive , later on painless. Microscopic features : Sections show vital pulp tissue with : 1- Chronic inflammatory cells ( plasma cells , lymphocytes) & some PMN leukocytes. 2- Granulation tissue commonly gets covered by epithelium as a result of implantation of epithelial cells on it is surface. 3- The epithelium is stratified squamous in type & closely resemble the oral mucosa even to the extent of developing well formed rete pegs & keratinized surface. Source of covering epithelium : i) Desquamated epithelial cells of the oral cavity carried by saliva . ii ) Rubbing against buccal mucosa , tongue or gingiva.
D ) Pulp necrosis & pulp gangrene : Untreated pulpitis may lead to death of the pulp. The inflammatory exudate compressed with a hard shell of dentine leads to compression of blood vessels particularly the apical , which then leads to infection & necrosis. The term pulp gangrene has been applied to this condition. Clinical features : clinically , necrosis is characterized by cessation of all symptoms . Microscopically : Microscopic section through such a tooth shows either an empty pulp chamber & canals or isolated areas of necrotic structureless masses. E) Pulp calcifications : They are : 1- pulp stones : developmental anomalies. 2- Diffuse calcification : * A morphous dystrophic calcification in the pulp. * Age degenerative changes. * No clinical significance except in endodontic treatment.
Pathology of periapical area -Periapical lesions are the end result of total pulpitis. -The periapical area is reached first by bacterial toxins & later by the micro-organisms. -The principle different types of periapical pathological lesions Bacterial causes Non-vital tooth Non-bacterial causes e.g. trauma Apical periodontitis Acute chronic Acute alveolar abscess periapical granuloma Acute osteomyelitis cellulitis Chronic abscess Radicular cyst Chronic osteomyelitis Associated changes i) Hypercementosis ii) Osteoeclerosis iii) Root resoption
Dental granuloma : ( chronic periapical periodontitis ) It is a localized mass of chronic inflammatory granulation tissue formed in response to infection. Location : classification according to the site 1- Periapical : due to spread infection from the pulp to periapical area. 2- Lateral : due to spread of infection from the pulp to the lateral surface of the root via accessory root canal. 3- Inter- radicular : when related to accessory root canal situated in bifurcation or trifurcation area. 4- Odontoiatrogenic : if the granuloma develops due to presence of artificial perforation made by the dentist during root canal treatment. Etiology : 1-low grade pulpitis. 2-Infection through deep periodontal pocket. 3-Trauma. 4-Haematogenous infection anchoresses phenomenon. 5-Odontogenic :
Acute apical periodontitis. In this early acute lesion inflammatory cells, mainly neutrophil polymorphonuclear leukocytes, are seen clustered around the apex of a non-vital tooth. The inflammatory cells are spreading around and into bone and there has not yet been time for significant bone resorption to develop. Oedema due to acute apical periodontitis. An acute periapical infection of a canine has perforated the buccal plate of bone causing oedema of the face; this quickly subsided when the infection was treated.
Chronic apical abscess. Periapical bone resorption has developed as a result of inflammation. The area of radiolucency corresponds with the histological changes seen in the next figure
* Deeply seated restoration * Use of unsterile root canal instruments. * Application of strong antiseptics in root canal therapy. Clinical features : 1- The involved tooth is sensitive to percussion. 2- Mild pain when biting or chewing. 3- The tooth feels slightly elevated (elongated) in it is socket. Pathogenesis: 1- First step is chronic pulpitis. 2- Pulp necrosis. 3- Extension of chronic inflammation into periapical periodontal ligament causing : i- Edema of periodontal ligament. Ii- Chronic inflammatory cell infiltration. 4- The body tries to wall off the infection by the formation of granulation tissue . 5-This tissue replaces the apical periodontal ligament. 6-Pressure of the growing granuloma causes bone resorption due to
increased osteoclastic activity. 7- As some of the periapical bone is destroyed , it gets replaced by granulation tissue , which become visible in X ray. Radiographic appearances : - Early : slight widening of periodontal ligament space. - Late : well circumscribed radiolucency of varying size. Histopathology : 1- Pulp of the affected tooth is necrotic or may shows chronic inflammatory cell infiltrate. 2- Alveolar bone proper & periodontal ligament in periapical area are replaced by granulation tissue. 3- This G.T. is surrounded by fibrous capsule. 4- Fibers of this capsule are attached to cementum of the root apex ( during extraction , granuloma is removed with tooth ) . 5- G.T. is consisted of : i) Young active fibroblasts. ii) Collagen fibrils. iii) Newly formed blood vessels with swollen endothelium. iv) Chronic inflammatory cells : Plasma cell + lymphocyte
6- Macrophages : histiocytes appear engulfing lipid material & are call foam cells. 7- Cholesterol crystals are seen in microscopic section as clefts due to dissolving of these crystals in alcohol & xylol during histological preparation. 8- Islands of epithelium : are often seen , the origin of which may be : i) Most commonly from epithelial rests of mallassez. ii) respiratory epithelium of maxillary sinus: as a result of perforating sinus wall or nasal floor. iii) oral epithelium : a) Growing from fistulous tract. b) From deep periodontal pocket. 9- When epithelial elements are so predominating in apical granuloma , the lesion is usually said to be ( epithelial root tumour) . 10- Proliferation of this epithelium will give rise to inflammatory periodontal cyst. 11- Acute exacerbation of apical granuloma will occur if the balance between the irritant & body resistance is disturbed ( acute or chronic abscess ).
Periapical abscess : It is an acute or chronic suppurative inflammation of periapical region. Sources : 1- Infection following pulpitis. 2- Trauma. 3- Pulp necrosis. 4- Haematogenous . 5- After root canal treatment . 6- Application of chemicals during root canal treatment. 7- Acute apical periodontitis follow acute pulpitis. 8- Most commonly an area of chronic infection on periapical granuloma. Clinical features: Local : 1) Extremely painful tooth. 2) Pain on percussion 3) Tooth is slightly extruded from it is socket. 4) Associated tooth usually shows : Deep carious cavity + deep restoration.
Low power detail shows the effects of apicectomy. The chronic inflammatory reaction has entirely cleared. New bone has formed to replace the excised apex and there is a condensation of connective tissue across the deep end of the root canal filling. Chronic periapical abscess. At the apex of the non-vital tooth is an abscess cavity surrounded by a thick fibrous wall densely infiltrated by inflammatory cells, predominantly neutrophils. Periapical bone has been resorbed and the trabeculae reorientated around the mass.
High power of an apical granuloma showing neutrophils, lymphocytes and plasma cells in loose oedematous fibrous tissue. Epithelial proliferation in an apical granuloma. Inflammation induces proliferation of odontogenic epithelium in rests of Malassez. This change may lead to cyst formation
5) The abscess may open intraoral or extraoral so decrease pain but still swelling increase 6) When pus escapes intraoral it may be : i) buccally ii) lingually General : systemic manifestation : - Swelling , pain , redness of overlying skin , lymphadenitis & fever Histopathology : 1) periapical tissue shows : i) dense masses of PMN leukocytes ( pus cells) . ii) spaces ( indicating areas from which pus was lost during histological preparation. 2) In periphery of the lesion , reduction in PMN leukocytes number occurs. 3) Bone trabeculae show empty lacunae due to death of osteocytes ( it is called sequestra.) Complications : 1) spread of infection either by : - Direct spread osteomyelitis -Haematogenous - Lymphatic
2) Spread along facial spaces to cause cellulitis or Ludwig,s angina 3) Gas gangrene ( due to presence of closteredium Welchii). 4) Embolic abscess in lung or brain. 5) Cavernous sinus thrombosis. 6) Maxillary sinusitis. Alveolar ostitis ( Dry socket ) : It is a localized non-suppurative ostitis of lamina dura after tooth extraction. Etiology : 1) Trauma by using great forces during extraction 2) Local anaesthesia 3) limited local blood supply 4) Osteosclerotic disease. 5) Radiotherapy. 6) Oral contraceptive. Pathogenesis : -Destruction of normal blood clot which is due to excessive local fibrinolytic activity or bacterial enzymes or both. - Bone damaged during extraction lead to local bone death. - Necrotic bone is separated by osteoclasts.
Clinical features : Age : usually adult , Sex: males more than females Site : lower premolars & molars Characters : 1) Painful socket ( Thrombbing aching pain) a few days after the extraction. 2) Breakdown or failure of the formation of the blood clot in the socket after extraction. 3) Bare bone. Treatment : - Relieving pain & promoting the healing by using irrigation & repeated dressing of socket ( Alvogel) . - Most cases relieved after one or two dressings. - Healing of the socket from it is base by granulation tissue. Prevention : Extraction should be carried out with minimal trauma.
Osteomyelitis It is an inflammation of the bone & bone marrow. Types : it is classified into 1) Acute 2) Chronic Etiology : 1) Local infection : alveolar abscess , alveolar osteitis, & infected cyst. 2) trauma from : extraction , compound fraction of jaw , & maxillofacial injury. 3) radiation damage. 4) Poorly controlled diabetes mellitus. 5) Malnutrition. Pathology : 1) Anerobic oral bacteria are important & also staphylococci. 2) The inflammation causes increased tension in the blood vessels of bone due to hyperemia : i) They cannot expand because surrounded by bone. ii) Pressure from surrounding edema fluid. iii) Haemo -concentration in them 3) Necrosis of the affected area of bone due to : cuts off the blood supply
from : i) the periosteum. ii) The adjacent normal bone 4) Then the necrosed bone becomes separated from the living by osteoclastic resorption of adjacent living bone. 5) A line of separation composed of granulation tissue is formed between necrosed & living bone, the separated dead bone is called squestrum & characterized by empty lacunae & deeply stained resting lines. 6) Bone marrow is replaced by infected material with pus. 7) Periosteal new bone formation ( due to the dilute irritant pus that acts as stimulant , this bone is first woven , it is called involucrum 8) The involucrum becomes perforated with holes called cloaca through which pus drains . Squestrum is hard , rough , light in weight & lighter in color than normal bone.
Acute osteomyelitis of the jaws Age : adult Sex : Males more than females Site : mandible more than maxilla Characters : • Severe pain & affected area is tender . • Numbness of the lower lip , if the inflammation spreads to the inferior dental nerve. • Swelling of the jaw ( oedema , pus & new bone formation ) . • The adjacent teeth become tender & loose. • When pus is formed it moves in various directions. • The pus perforates the bone & reaches to the soft tissues, resulting in swelling & redness of soft tissue ( inflammation). • Then the pus discharged by perforating the oral mucosa or skin forming sinuses. • The acute osteomyelitis become chronic when the sinuses are formed ( draining the pus) . • By passing probe into the sinus , you can feel bare bone which is rough when necrosis is resulted & loose when sequestrum is formed. • The regional lymph nodes become enlarged & tender . • Rigors & pyerxia , fever & leukocytosis in acute phases.
Radiographic Features : -During the first two weeks , there is no changes in radiographs. - Later on , irregular rdaiolucent areas develop & have moth or worm – eaten appearance , with small squestra which appear slightly more radio – opaque than the normal bone. - Sub – periosteal new bone formation . Treatment : 1) Drain the pus , & pus smear is taken for culture for i) Determination of the causative micro-organisms . ii) test the micro-organisms sensitivity to antibiotics. 2) Vigorous antibiotics. 3) Drainage. 4) Establishing a good oral hygiene & use saline mouth bath. 5) Analgesics. 6) remove source of infection. 7) Remove bone when squestrum is formed . 8) Decortication if necessary.
Chronic osteomyelitis Types of chronic osteomyelitis : 1) Chronic suppurative osteomyelitis. 2) Chronic focal sclerosing osteomyelitis. 3) Chronic diffuse sclerosing osteomyelitis 4) Chronic non-suppurative osteomyelitis. • Chronic suppurative osteomyelitis : - This may be a sequela of inadequate treated acute osteomyelitis , or chronic osteomyelitis arise de novo. Clinical features : Age : adult , Sex : Males more than females. Site : Mandibular molar area is the most affected region. Characters : swelling of the jaw , loose teeth , sinus tract drain pus from the jaw , mild pain , mild fever , blood picture moderate leukocytosis , the symptoms are of long duration.
Histopathology : 1) Chronic inflammatory cells infiltrating a fibrous bone marrow. 2) Irregular bone trabeculae with many reversal lines ( osteoblastic & osteoclastic activities) . 3) Sequestra ( Necrotic one ). 2) Chronic focal sclerosing osteomyelitis: Other name : condensing osteitis. Uncommon bony reaction to low grade periapical inflammation or due to strong local tissue resistance . Clinical features : Age : under 20 year Sex : both. Site : mandibular molars ( non vital & carious teeth). Radiographic : Radio-opaque area 2-3cm in diameter below the apex of the roots. Histopathology : -Formation of dense compact bone with empty lacunae. -Chronic inflammatory cells. Treatment : Removal of the offending tooth followed by slow resolution.
3) Chronic diffuse sclerosing osteomyelitis: Age : Old age Sex : equal Site : Bilateral molar region Race : blacks Characters : Vague pain , unpleasent taste , mild suppuration , & fistula formation . Radiographic : diffuse or nodular radio=opacities. Histopathology : Chronic inflammatory cells, dense irregular bone formation with reversal lines resemble other sclerotic bone diseases. Treatment : removal of any infected teeth , antibiotics & removal dense masses after squestration.