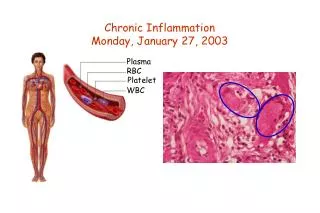
Chronic Inflammation
Chronic Inflammation. Dr Rezaur Rahman. Learning objectives for PMDC in Chronic Inflammation. Chronic inflammations/ Granulomatous diseases. The systemic effects of acute and chronic inflammation and their possible outcomes. Significance of ESR.

Chronic Inflammation
E N D
Presentation Transcript
Chronic Inflammation Dr Rezaur Rahman
Learning objectives for PMDC in Chronic Inflammation • Chronic inflammations/ Granulomatous diseases. • The systemic effects of acute and chronic inflammation and their possible outcomes. • Significance of ESR. • Examples of induced hypothermia in medicine. • Pathogenesis, clinical features and lab. Diagnosis of Gout. • Management of acute and chronic Gout.
Definition of Chronic Inflammation Inflammation of prolonged duration (weeks or months) in which active inflammation, tissue destruction and attempts at repair are proceeding simultaneously
Aetiology: Onset & Causes A. Chronic inflammation from onset (de novo) • Persistent infection by certain microorganism • Prolonged exposure to toxic/aggressive agent • Autoimmunity: RA, SLE, Hashimoto’s thyroiditis, Chronic gastritis of pernicious anaemia • Unknown cause: Sarcoidosis, Crohn disease, ulcerative colitis B. Chronic inflammation developing from acute inflammation(Acute to Chronic)
A. Chronic inflammation from onset (de novo) • Persistent infection by certain microorganism • Prolonged exposure to toxic/aggressive agent • Autoimmunity: RA, SLE, Hashimoto’s thyroiditis, Chronic gastritis of pernicious anaemia • Unknown cause: Sarcoidosis, Crohn disease, ulcerative colitis
1.Persistent infection by certain microorganism • Mycobacterium tuberculosis, Mycobacterium lepri, Treponema pallidum, certain viruses, fungi, parasite- low toxicity, delayed hypersensitivity and granulomatous inflammation • Helicobacter pylori- Chronic gastritis, gastric ulcer, duodenal ulcer
2.Prolonged exposure to toxic/aggressive agent • Aggressive action of acid pepsin in gastric juice causing peptic ulcer • Cigarette smoking causing Chronic bronchitis • Toxic plasma lipid components- atherosclerosis • Talc, suture, other nondegradable material • Silica- silicosis of lung
B. Chronic inflammation developing from acute inflammation(Acute to Chronic) • Persistence of injurious agent, eg, organism in abscess • Interference in healing process, eg, sequestrum(dead bone) in chronic suppuratve osteomyelitis • Drainage is delayed or inadequate, eg, lung abscess • Recurrent bouts of acute inflammation, eg, chronic pyelonephritis, chronic cholecystitis, chronic gout.
Histological types of Chronic Inflammation • Specific Chronic Inflammation: histologically distinctive. Granulomatous inflammation is specific inflammation • Nonspecific Chronic Inflammation: not histologically distinctive
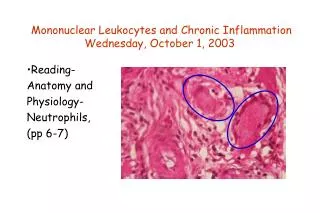
Granuloma: • Granuloma is a microscopic aggregation of macrophages and epitheloid cells which are modified macrophages, surrounded by a collar of mononuclear leucocyte, principally lymphocyte. Usually giant cells and occasionally plasma cells are present.
Giant cell of Granuloma: • Large cell with more than one nucleus. • Formed by fusion of macrophages or epitheloid cell. 20 or more small nuclei are present. • Types: • Langhans’ giant cells- nuclei are arranged in horse-shoe pattern. Found in tuberculosis and sarcoidosis • Foreign body giant cells- haphazardly scattered nuclei. Found in foreign body granuloma. • Aschoff giant cell- rheumatic lesion • Giant cell of ‘Giant cell tumor of bone’- osteoclast type • Tuton giant cell- in Xanthoma • Giant cell to reaction to sodium urate crystal in gout ** Physiological Giant cell- Osteoclast, megakaryocyte etc
Malignant giant cell: Found in- • Anaplastic tumor • Hodgkin’s disease: Reed-Stenberg giant cell • Choriocarcinoma • Poorly differentiated astrocytoma
Classification of Granulomatous inflammation • Aetiologicalclassification • Infectious agent- bacteri, helminth, fungi • Physical & chemical agents- exogenous & endogenous • Autoantigen: Wegener’s grnulomatosis, Giant cell arteritis • Unknown: Sarcoidosis, Crohn’s disease • Classification on Pathogenesis • Immune granuloma • Foreign body granuloma • Histological classification • Non caseatinggranuloma • Caseatinggranuloma • Suppurative granulomatous inflammation • Diffuse granulomatous inflammation
A. Infectious agent • Bacteria: • Mycobacterium tuberculosis- tubercle- noncaseating/hard & caseating/soft • Mycobactrium lepri- tuberculoid & lepromatous • Treponema pallidum- Gumma • Helminth: • W. bancrfti • A. lumbricoides • Schistosoma • Fungi: • Rhinosporidiosisseeberi • Cryptococcus neoformans, Coccidioidoimmitis & Histoplasmacapsulatum
Nonspecific chronic Inflammation • Chronic inflammatory ulcer- peptic ulcer • Chronic suppuratve inflammation- chronic abscess, chronic pyelonephritis, chronic osteomyelitis • Chronic fibrinous, serous or serofibrinous inflammation following acute inflammation • Chronic catarrhal inflammation- chronic allergic rhinitis • Chronic necrotizing inflammation- chronic amoebiasis
Systemic effects of Acute Inflammation • Fever: • Leucocytosis, specially neutrophilicleucocytosis- due to stimulation of bone marrow leading to release of immature cells in the circulation(shift to the left) • Synthesis of ‘acute phase protein’- liver synthesizes acute phase protein like C reactive protein(CRP), Fibrinogen and Serum Amyloid A(SAA). CRP is a marker of activity and very useful prognostic test for active Rheumatic fever and other conditions where there is increased tissue necrosis like MI. As it is not influenced by other factors, so it is more useful than ESR. Increased Fibrinogen level is responsible for high ESR. SAA is responsible for deposition of amyloid in different tissues • Others- lethargy, anorexia, sweating, tachycardia, hypotension, hypoglycaemia leading to shock due to liberation of different cytokines, particularly IL1, TNF.
Systemic effects of Chronic Inflammation • Fever • Anaemia • Leucocytosis- lympho or monocytosis • ESR- elevated • Amyloidosis