Chronic inflammation
Chronic inflammation. By Dr. S Homathy. Chronic inflammation. Inflammation of prolonged duration(weeks to months to year) In which acute inflammation, tissue injury and healing proceed simultaneously. Components of chronic inflammation. 1.Acute inflammation 2.Demolition


Chronic inflammation
E N D
Presentation Transcript
Chronic inflammation By Dr. S Homathy
Chronic inflammation • Inflammation of prolonged duration(weeks to months to year) • In which • acute inflammation, • tissue injury and • healing • proceed simultaneously
Components of chronic inflammation 1.Acute inflammation 2.Demolition 3.Healing – repair and regeneration 4.Immune response
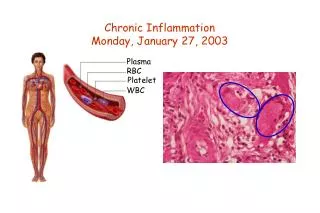
It is characterized by • Infiltration with mononuclear (‘chronic inflammatory’) cells, including • Macrophage • Lymphocytes • Plasma cells • Tissue destruction • Largely directed by inflammatory cells • Repair • Involving new vessel proliferation( angiogenesis and fibrosis)
1.Acute inflammation • Evidence of acute inflammation is frequently seen in chronic inflammation Eg: pus rich in neutrophils in osteomyelitis, pyonephrosis, chronic brain abscess : exudates rich in Eosinophils in hypersensitivity reaction • 2.Demolition • Accomplished by macrophages derived from emigrating monocytes of bone marrow origin
3.Healing • Repair • New vessel formation (angiogenesis) • Fibrosis (dense fibrosis and loss of function) • Regeneration • Clearance of injurious stimuli • Clearance of mediators and chronic inflammatory cells • Regeneration and remodeling of damaged tissue • Normal function Eg : surface epithelia
4.Immune response • Very common feature is the accumulation of lymphocytes of various types, plasma cells, and MP. • Plasma immunoglobins levels may be elevated.
Chronic inflammation can occur • Following acute inflamation or • Starting de novo
Differ from AI • Absence of cardinal signs • New vessel formation • No fluid exudation or oedema • Time is prolonged • Immune response • Injurious agents most often cause insidious, progressive and often extensive tissue necrosis • Accompanied by ongoing repair by fibrosis • Specific ( immune response is activated) • Systemic response – low grade fever, weight loss, anaemia
Causes of chronic inflammation • Viral infections • Intracellular infection of any kind require lymphocytes and macrophages • To identify and eradicate infected cells. • Persistent microbial infections • By some specific organisms Eg: Mycobacteria, Treponemapallidum, certain fungi • Organisms are low direct pathogenicity • Typically evoke an immune response- delayed hypersensitivity
Persistent injury • Prolonged exposure to potentially toxic agents Eg : silica produce -silicosis of lung : chronically elevated plasma lipids- produce Atherosclerosis • Autoimmune diseases • Immune response to self- antigen and tissues Eg: Rheumatoid arthritis / multiple sclerosis.
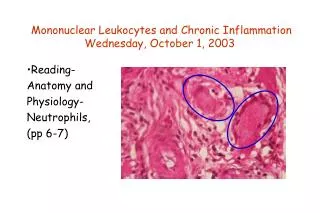
The Players (mononuclear phagocyte system) • Macrophages • Scattered all over • Microglia - CNS • Kupffer cells - liver • sinus histiocytes– spleen , lymphnode • alveolar macrophages - lungs. • Circulate as monocytes • reach site of injury within 24 – 48 hrs and transform into large macrophages • Large MP now capable of phagocytosis
Become activated by T cell-derived cytokines, endotoxins, and other products of inflammation • Greater ability to kill ingested organisms LM appearance with H&E stain • Large • Flat • Pink • Similar to squamous cell ( called epithelioid macrophages)
After activation, MP secretes a wide variety of biologically active products • If unchecked leads to tissue injury and fibrosis • Mediaters from MP • Acid and neutral proteases • Complement and coagulation factors • C1 to c5 • Propedin • Coaguulation factor V and VIII • Reactive oxygen speces and NO • AA metabolites • CK
In CI MP accumulation persist and MP can proliferate • lymphocytes derived factors recruit or immobilize the MP to the site of injury • IL-4 or INF-γ • Causes MP to fuse into large, multinucleated cells • Called giant cells
T and B lymphocytes • Antigen-activated (via macrophages and dendritic cells) • Release macrophage-activating cytokines (in turn, macrophages release lymphocyte-activating cytokines until inflammatory stimulus is removed) • Plasma cells • Terminally differentiated B cells • Produce antibodies
Eosinophils • Found especially at sites of parasitic infection, or at • allergic (IgE-mediated) sites • Mast cells • Participate in both acute and chronic inflammatory responses • Armed with IgE to certain antigens
Chronic endometritiswithlymphocytes as well as plasma cells in the endometrial stroma. • In general, the inflammatory infiltrate of chronic inflammation consists mainly of mononuclear cells ("round cells"): • lymphocytes, plasma cells, and macrophages.
Chronic cervicitis. • Prolonged acute inflammation or repeated bouts of acute inflammation may lead to the appearance of • more mononuclear cells, • and chronic inflammation. • In this case the inflammation is severe enough to produce mucosal damage with hemorrhage.
Chronic inflammation can go on for a long time: • weeks to months to years. • Seen here in the synovium from the joint of a patient with rheumatoid arthritis are • collections of dark blue lymphocytes.
Types of chronic inflammation • Granulomatous chronic inflmmation • Non- granulomatous chronic inflammation
Granulomatous inflammation Definition: • Granulomatous inflammation is a distinctive pattern of chronic inflammatory reaction. • It is a protective response to chronic infection or foreign material, preventing dissemination and restricting inflammation. • Some autoimmune diseases such as Crohns disease is also associated with granulomas.
Cellular constituents of Granulomas • the predominant cell type is an activated macrophage with a modified epithelial-like (epithelioid) appearance • Lymphocytes. • Occasional plasma cells
What Is A Granuloma? • A granuloma is a microscopic aggregation of macrophages that • are transformed into epithelium-like cells surrounded by • a collar of mononuclear leukocytes, • principally lymphocytes and occasionally plasma cells. • Older granulomas also develop a surrounding rim of fibroblast and connective tissue • Due to CK elaborated by the activated MP • Frequently, but not invariably multinucleated giant cells are also found • Derived from fusion of 20 or more MP
These are epithelioid cells around the center of a granuloma. • They get their name from the fact that they have lots of pink cytoplasm similar to squamous epithelial cells. • Their nuclei tend to be long and stringy
Epithelioid cells fuse to form giant cells containing 20 or more nuclei. • These giant cells can be found either at the periphery or the center of the granuloma
Types of giant cells • The nuclei arranged either • Peripherally • Langhans-type giant cell (Reaction to certain organism) • haphazardly • foreign body-type giant cell (reaction to insoluble materials)
Nuclei enclose the central part of the homogeneous eosinophilic cytoplasm and the peripheral part of the cytoplasm is vacuolated due to its lipid content • Touton giant cell (found in xanthomas)
MP found in Rheumatic heart disease also called caterpillar cells, as they have a large amount of clear cytoplasm surrounding a rod-shaped nucleus that to some resembles a caterpillar. • Larger Anitschkow cells may coalesce to form multinucleated Aschoff giant cells
Nuclears appears as amirror image of one another • Reed-sternberg giant cell found in Hodgkin’s lymphoma
Fibrous connective tissue often surrounds granulomas (remodeling of tissue) • Areas within the granulomacanundergo necrosis • prototype: caseous necrosis in tuberculosis. • Granular, cheesy • Necrosis can lead to calcification or liquefaction and formation ofa cavern if drained.
CAUSES OF GRANULOMATOUS DISEASES Infectious causes: • Bacteria • Tuberculosis • Leprosy(tuberculod type) • Trepanemapallidum • Brucella species • Rickttsial organism • Coxiellaburnetii • Parasites • Schistosomiasis
Fungi • Histoplasmosis • Blastomycosis • coccidioidomycosis Metal/Dust • Berylliosis • Silicosis
Foreign body Granulomas: • endogenous ( keratin, necrotic bone or adipose tissue uric acid crystals) • Exogenous (wood, silica, asbestos, silicone,suture…) • Specific chemicals: • Beryllium • unknown cause • Sarcoidosis • Crohn’s disease
Type of granulomas • Foreign body granulomas • form when material such as talc, sutures, or other fibers are large enough to preclude phagocytosis by a single macrophage.
2. Epithelioidgranuloma (Immune granulomas ) • caused by insoluble particles that are capable of inducing a cell-mediated response. • This type of immune response produces granulomas when the inciting agent is poorly soluble or particulate.
Macrophages • engulf the foreign material and • process and • present some of it to appropriate T lymphocytes, • causing them to become activated, • responding T cells produce cytokines, • such as IL-2 • which activates other T cells and • IFN- • which is important in transforming macrophages into epithelioid cells and multinucleate giant cells.
Here is a foreign body type giant cell at the upper left of center • adjacent to a segment of vegetable material aspirated into the lung. • Such foreign body giant cells have nuclei scattered haphazardly about the cell
Two foreign body giant cells are seen • just to the right of center • where there is a bluish strand of suture material from a previous operation
Granulomatous disease can become quite extensive. • Here are numerous confluent granulomas in upper lung fields in a case of active pulmonary tuberculosis.
Grossly, • a granuloma tends to be a focal lesion. • Seen here in a hilar lymph node is a granuloma. • Granulomas due to infectious agents such as mycobacteria are often described as "caseating" when they have prominent caseous necrosis.
The focal nature of granulomatous inflammation of lung • in which there are scattered granulomas in the parenchyma. • This is why the chest radiograph with tuberculosis or other granulomatous diseases is often described as "reticulonodular". • A biopsy could miss such lesions from sampling error, too.
Giant cells are a "committee" of epithelioid macrophages. • Seen here are two Langhans type giant cells in which the nuclei are lined up around the periphery of the cell. • Additional pink epithelioid macrophages compose most of the rest of the granuloma
This is a caseatinggranuloma. • Epithelioid cells surround a central area of necrosis that appears • irregular, • amorphous, and pink. • Grossly, areas of caseation appear cheese-like
Granulomas caused by • tuberculosis and • pathogenic fungi such as • Histoplasmacapsulatum or Cryptococcus neoformans • are often caseating. • Here, the area of caseation is seen at the upper right.