Download
1 / 26
260 likes | 264 Vues
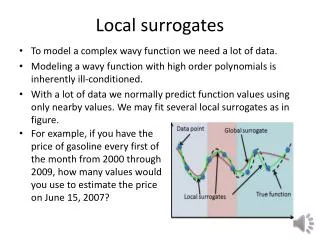
Biomarkers as Surrogates Tipping the Balance Toward Persuasiveness. EveryLife Foundation Rare Disease Workshop May 2013 Washington, DC Marc K Walton MD, PhD Associate Director for Translational Medicine Office of Translational Sciences CDER-FDA.

E N D
Biomarkers as SurrogatesTipping the Balance Toward Persuasiveness EveryLife Foundation Rare Disease Workshop May 2013 Washington, DC Marc K Walton MD, PhD Associate Director for Translational Medicine Office of Translational Sciences CDER-FDA The views expressed are those of the author, and do not necessarily represent an official FDA position
Biomarkers in A&WC Studies (Phase 3) Secondary endpoint Supportive of primary EP findings Objective, precise Helps decrease uncertainties regarding primary efficacy endpoint results interpretation Primary Endpoint Surrogate endpoint for a specific Context of Use Well established relationship to clinical outcome Conventional marketing approval “reasonably likely to predict…” relationship Accelerated approval provisions of regulations
Surrogate Endpoint Stands in place of an efficacy endpoint Feels Functions Survives Usually intended as a prediction of a future clinically meaningful outcome Requires assumptions about future clinical course after biomarker measurement with continued drug treatment
Questions for Evaluation – Disease Related Do we know the underlying primary cause? True single etiology or multiple closely related etiologies or syndrome with (potentially) different etiologies? How well do we understand the complete pathophysiology from primary cause to meaningful clinical outcome? How detailed is the knowledge? How strongly do we believe our “knowledge” (interpretation of scientific observations) is complete and correct? What is nature of variation in disease? Homogeneous / broadly heterogeneous / heterogeneous with distinct, homogeneous, phenotypes? How well understood is the basis for the variation?
Questions to Consider – Biomarker Focus What is the physiologic concept thought related to clinical outcome? How should that concept be measured? The biomarker is this measurement What clinical outcome is it expected to predict? When is the clinical outcome expected? Relative to the measurement of the biomarker Is the biomarker in the direct pathophysiologic pathway leading to that clinical outcome? Versus a side branch How confidently understood? (refer to ‘disease related’ issues)
Is it in a unitary part of the pathophysiologic pathway leading to the clinical outcome? Versus in one of several parallel pathologic pathways Where in the sequence of pathophysiologic steps does the biomarker occur? Do we know the anatomic location where the biomarker functions in the disease process? Is the biomarker being sampled at the site where it functions in the pathophysiology? If not, how do measurements at the site of sampling relate to effects at the site of function? Issues for Evaluation – Biomarker Focus
Issues for Evaluation – Biomarker Focus How close in the pathopysiologic sequence is the biomarker to the intended clinical outcome? What is the shape of the biomarker – clinical outcome relationship? Does the change observed in the biomarker lead to a meaningful change in the clinical outcome? Amount of change in each Location of that change within the full scale of the biomarker Major question Dynamic range of biomarker
Questions to Consider – Drug-related How certain are we of the mechanism of drug action? Where in the pathophysiology sequence does the drug act? Relationship to biomarker’s location in the pathophysiology What is known about the time course relationship of drug administration (or readministration) and effects on the biomarker? When should the biomarker be sampled? What are the assumptions about drug effect over time between biomarker sampling and clinical outcome?
Additional supportive information Other biomarkers Measure steps in pharmacology/ pathophysiology prior to or after primary biomarker Are effects on those biomarkers consistent with expected relationships Clinical effect observations Clinical effects of uncertain meaningfulness Underpowered meaningful clinical endpoints with concurrent trend in outcome
Potential Sources of Information Clinical trials of specific drug candidate Biomarker – Clinical relationship Clinical trials of other interventions Same or different mechanism Understanding of disease pathophysiology and relationship to clinical course – Natural history Understanding of normal human physiology Information from related diseases Animal models of the disease Pathophysiology Biomarker relationship Treatment effects on biomarker and clinical measures Phenotype relevance of the model(s)
Potential Hazards of Relying on Surrogate Endpoint Failure of surrogate’s prediction False indication of presence of benefit Misleading prediction of amount of benefit Limited safety experience may be inadequate Dataset often more limited than with clinical endpoint studies Real risks of drug may not be observed “Off-target” effects of drug may occur later than biomarker measurement Potential use of a drug with an unfavorable benefit-risk comparison
Accepting a Biomarker as a Surrogate Consider all issues Multiple issues Importance of each varies case to case Consider all available relevant information Multiple kinds of information Strength of different kinds of information varies Relevance to different issues Strengths and weaknesses of available information Consider key types of information absent Importance of missing information varies case to case Central problem – What makes for a persuasive body of information? Prior cases as guiding examples
Informative Examples Acute MI Arterial blood flow Alpha1-antitrypsin Deficiency Enzyme Levels Phenylketonuria Phe blood level Fabry Disease Renal capillary endothelial histology MPS 1 Urinary GAG Transfusional hemosiderosis Liver iron content
Informative Examples (2) Fractures in Osteoporosis Bone mineral density with fluoride Mortality in Acute MI PVCs with antiarrythmic agents (CAST) Stroke, MI, death in Cardiovascular Disease HDL with torcetrapib Infections in Chronic Granulomatous Disease Superoxide with Interferon gamma Arthritis in Gout Serum uric acid with multiple drug classes
Acute MI Clinical outcome is mortality Intravenous thrombolytic agent is the treatment Biomarker is the concept of blood flow (patency) How and when is blood flow evaluated? Development of reteplase (R-PA) RAPID-2 Study Evaluated biomarker GUSTO-III Study Evaluated clinical outcome
Acute MI R-PA superior to T-PA Irrespective of which amount or when the concept of blood flow is assessed
Acute MI Concept indicating efficacy is blood flow How and When should it be measured? What is the shape of the relationship?
Understanding the Surrogate Measure: Idealized Drug Drug Drug Drug Intervention Intervention Intervention Intervention Pathophysiologic Pathophysiologic Clinical Clinical Clinical Clinical Surrogate Surrogate Surrogate Surrogate Processes Processes P2 P2 P2 P2 P1 P1 P1 P1 Outcome Outcome Outcome Outcome Endpoint Endpoint Endpoint Endpoint Order of Processes
Understanding the Surrogate: Silent Surrogate Drug Drug Intervention Intervention Pathophysiologic Pathophysiologic Clinical Clinical Surrogate Surrogate Processes Processes P2 P2 P1 P1 Outcome Outcome Endpoint Endpoint Order of Processes
Understanding the Surrogate: Complexity Drug Drug Intervention Intervention Surrogate Surrogate Endpoint Endpoint P2 P2 Clinical Clinical P1 P1 Outcome Outcome P3 P3 Order of Processes
Shape of the Surrogate - Clinical Relationship Clinical Status Biomarker
Clinical – Biomarker Relationship Good C1 C2 C3 Clinical Status C6 C4 C5 Poor Low Biomarker High
Clinical Effects of Biomarker Change Good C3 Clinical Status C1 C2 Poor b1 b2 Low High Biomarker
Clinical – Biomarker Relationship Good Clinical Status C1 C3 C2 Poor Low Biomarker High
Accelerated Approval Should be a goal only after careful thought Plan how to show “reasonably likely to predict” Plan how to verify clinical benefit Difficulty of verification may be increased in rare diseases Mistaken belief in efficacy has disadvantages Patient burden from treatment without benefit Effort, ‘side effects’ (moderate, common AE), cost Safety risk without benefit May be impediment to develop a second treatment, which might be truly efficacious
Confirmatory Study Develop plan by mid-way in development program Also an A&WC study “Usually underway” at time of AA Multiple approaches As extension of primary biomarker study In closely related population Dose comparison study



![[PDF] DOWNLOAD FREE Tipping Toward Balance: A Fitness Trainer's Guide to Stabili](https://cdn7.slideserve.com/12581032/tipping-toward-balance-a-fitness-trainer-s-guide-dt.jpg)