Rubella Virus
Rubella Virus. A Microbiology Presentation By Bernadette Rolle. Table of Contents. Introduction Replication Cycle Transmission and Epidemiology Pathogenesis and Immunity Clinical findings Lab Diagnosis Treatment Prevention Reference. Introduction.

Rubella Virus
E N D
Presentation Transcript
Rubella Virus A Microbiology Presentation By Bernadette Rolle
Table of Contents Introduction Replication Cycle Transmission and Epidemiology Pathogenesis and Immunity Clinical findings Lab Diagnosis Treatment Prevention Reference
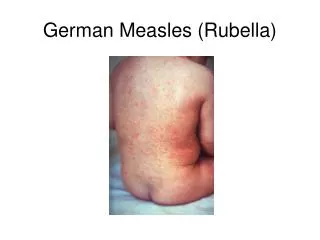
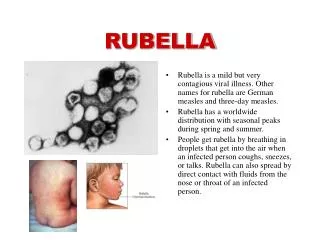
Introduction Rubella, commonly known as German measles, is a disease caused by the rubella virus. The name derived from the Latin, meaning “Little Red”. Called German measles because it was first described by German Physicians in the mid-eighteenth Century. This disease is mild and often when it attacks, it passes unnoticed. It can last from one-three days
Definition Acute onset of generalized maculopapular rash Temp. >37.2C(99F) if measured Arthritis/Arthralgia and lymphodenopathy and or conjunctivitis
Virus attaches to host cell. Plasma membrane surrounds the virus and an endosomal vesicle forms. The envelope of the virus fuses with the membrane and the vesicle. The virus is released into the host's cytoplasm Viral nucleic acid separates from its capsid Nucleic acid enters host nucleus and replicates Transcription into mRNA Host ER directed by mRNA to synthesize glycoproteins and capsid proteins plus proteins of the viral envelope. Vesicles transport glycoproteins to plasma membrane of cell. New viruses assemble and are released from host cell after being enveloped by host's modified plasma membrane. REPLICATION CYCLE
Mode of transmission Rubella is transmitted by droplet spread or direct contact with infectious patients. Can also be spread across the placenta from mother to fetus
Epidemiology Rubella and the congenital rubella syndrome (CRS) have largely been eliminated in the united States. The incident of rubella has declined from 0.45 per 100,000 in 1990 to 0.1 per 100,000 in 1999. However rubella out break continues to occur in other parts of the world, and CRS remains a concern. Prior to the introduction of the rubella vaccine in 1969, epidemic appeared in 6-9 years cycles, usually in the late winter and early spring. In 1964, a major worldwide pandemic spread to the United States resulting in approximately 12.5 million cases, as many as 11,000 fetal deaths and approximately 20,000 cases of congenital rubella syndrome
1969 and 1970 Attenuated rubella vaccines licensed in USA and UK (USA universal childhood programme; UK selective vaccination of prepubertal school girls)6 1971 MMR licensed in USA 1978, 1979, and 1983 Severe UK rubella epidemics 1988 UK policy augmented by offering MMR to preschool children of both sexes
1989 USA introduced a two-dose measles vaccination at age 12–15 months and at age 4–5 years or 11–12 years 1989–91 Resurgence of rubella in USA 1996 In UK, schoolgirl vaccination discontinued but second dose of MMR introduced for children aged 4–5 years 2000 WHO organized first global meeting on rubella since 1984 2002 123 (57%) of 212 of countries and territories include rubella vaccination in national immunisationprogrammes
Pathogenesis • Spread by droplet from (7-10 days before rash) • Incubation period 14 days (range 12-21) • Virus replication in nasopharynx and lymphoid tissue. •lymphatic system leading to Viraemia (via the blood stream) and systemic infection, Where it makes its appearance on the skin. The rash is attributed to the viral replication and immune injury During maternal infection, it replicates in the placenta then spread to fetal tissue.
Immunity Antibody is generated after the viremia, and its appearance correlates with the appearance of the rash. The antibody limits viremic spread, but cell-mediated immunity plays an important role in resolving the infection.
Maternal IgG does not transfer efficiently in the first trimester; therefore, fetal blood levels of IgG are only 5% to 10% of maternal levels. On the other hand, maternal IgG protects the fetus from anomalies in the second and third trimesters. The fetus produces its own antibodies in late pregnancy, when levels may exceed those in maternal serum. Infection rates and the risk of congenital rubella syndrome are highest during the first trimester. The risk of fetal infection varies between maternal primary infection and reinfection.
Clinical Findings Children generally have few symptoms. Adults may experience a fever, headache, general discomfort (malaise), and a runny nose before the rash appears. They may not notice the symptoms. Other symptoms may include: Bruising (rare) Inflammation of the eyes (bloodshot eyes) Muscle or joint pain If a woman is found to be pregnant during her infection, the 1st trimester is the critical trimester.
Congenital rubella syndrome Cataracts/congenital glaucoma, congenital heart disease (most commonly patent ductusarteriosus or peripheral pulmonary artery stenosis), loss of hearing, pigmentary retinopathy. Purpura, splenomegaly, jaundice, microcephaly, mental retardation, meningoencephalitis, radiolucent bone disease.
Laboratory Findings • Serology • In primary rubella infection, the appearance of clinical symptoms is associated with the appearance of both IgG and IgM antibodies • IgM antibodies – detectable a few days after onset of symptoms; peak 7-10 days later • May consider fetal IgM serology if fetal infection suspected indicating previous infection and immunity • Prenatal screening – test women prior to pregnancy to confirm presence of IgG antibodies indicating previous infection and immunity
Polymerase Chain reaction (PCR) • Usually throat or urine samples • Amniotic fluid when fetus is at least 2 weeks of age to identify fetal infection
As with the measles and most other viral illnesses, there's no cure for Rubella. You can only wait for it to go away. Analgesics such as acetaminophen* and ibuprofen can control fever and headache and joint pains. Immunize Per WHO schedule 12mths then 15mths then between ages 4-5 years If uncertain of immunization and one is planning pregnancy, council with your Dr. to ensure you and yours are protected.
References http://en.wikipedia.org/wiki/Rubella_virus http://www.cdc.gov/rubella/ http://www.who.int/mediacentre/factsheets/fs367/en/ http://www.cdc.gov/vaccines/pubs/surv-manual/chpt15-crs.html
The End THANK YOU FOR BEING SOOOO ATTENTIVE!!!!