
RUBELLA
E N D
Presentation Transcript
What is Rubella Rubella is a disease caused by the rubella virus. Rubella is usually a mild illness. Most people who have had rubella or the vaccine are protected against the virus for the rest of their lives. Because of routine vaccination against rubella since 1970 , rubella is now rarely reported.
Rubella( German Measles ) Rubella is also called as 3 day Measles or German Measles. Family – Togaviridae Genus - Rubivirus In general belong to Togavirus group
Rubella Virus Rubella virus are ss +ve RNA virus Diameter 50 – 70 nm Enveloped Spherical Virus carry hemagglutinin Virus multiply in the cytoplasam of infected cell.
Culturing the Virus The virus can be cultured and adopted to continuous cell lines Rabbit kidney cells (RK 13 ) and Vero cells
Main Clinical Events The clinical events occuring in the neonatal age is more important and divided into two major groups 1 Post Natal Rubella 2 Congenital Rubella
How Adults acquire Infection Acquired, (i.e. not congenital), rubella is transmitted via airborne droplet emission from the upper respiratory tract of active cases. The virus may also be present in the urine, feces and on the skin. There is no carrier state: the reservoir exists entirely in active human cases. The disease has an incubation period of 2 to 3 weeks.
Post natal Rubella Occurs in Neonates and Childhood Adult infection occurs through mucosa of the upper respiratory tract spread to cervical lymphnodes Viremiadevlops after 7 – 9 day Lasts for 13 – 15 days Leads to development of antibodies The appearance of antibodies coincides the appearance of suggestive immulogic basis for the rash In 20 – 50 % cases of primary infections are subclinical
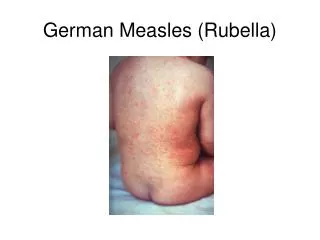
Clinical findings Malaise Low grade fever Morbilliformrash Rash starts on Face Extremities Rarely lasts more than 5 days No features of the rash give clues to definitive diagnosis of Rubella.
Rubella Rashes When epidemics occur with similar features it is more suggestive of Rubella epidemics Other Enterovirus infections can produce similar manifestations.
Other manifestations and complications May produce transient Arthritis, in women in particular. Serious complications are Thrombocytopenia Purpura Encephalits
Immunity - Rubella Antibodies appear in serum as rash fades and antibody titers raise Rapid raise in 1 – 3 weeks Rash in association with detection of IgM indicates recent infection. IgG antibodies persist for life
Immunity - Protects One attack of Rubella infection, protects for life Immune mothers transfer antibodies to off springs who are in turn are protected for 4 – 6 months.
Diagnosis of Rubella in Adults Clinical Diagnosis is unreliable Many viral infections mimic Rubella Specif diagnosis of infection with 1 Isolation of virus 2 Evidence of seroconversion
Isolation and Identification of virus Nasopharyngeal or throat swabs taken 6 days prior or after appearance of rash is a good source of Rubella virus Using cell cultured in shell vial antigens can be detected by Immunofluresecentetmehods
Serology In Rubella Hemagglutination inhibition test for Rubella is of Diagnostic significance ELISA tests are greater importance A raise in Antibody titers must be demonostrated between two serum samples taken at least 10 days apart. Or Detection of Rubella specific IgM must be detected in a single specimen.
Epidemiology Rubella is world wide in distribution Occurs round the year, Epidemics occur every 20 – 25 years Infection is transmitted by respiratory route The use of Rubella vaccine has now eliminated both epidemic and endemic Rubella in USA and several developed countries
Treatment and Prevention Rubella is a mild self limited illness. No specific treatment or Antiviral treatment is indicated. However Laboratory proved and clinically missed Rubella in the Ist 3-4 months of pregnancy is associated with fetal infections.
Congenital Rubella Syndrome Maternal viremia with Rubella infection during pregnancy may result in infection of placenta and fetus. The growth rate of fetal cells are reduced. Results in fewer number of cells after the birth. Lead to deranged and hypo plastic organ development. Results in structural damage and abnormalities
Rubella infection – At various trimesters Ist trimester infections lead to abnormalities in 85 % of cases. and greater damage to organs 2nd trimester infections lead to defects in 16 % > 20 weeks of pregnancy fetal defects are uncommon However Rubella infection can also lead to fetal deaths, and spontaneous abortion. The intrauterine infections lead to viral excretion in various secretion in newborn upto 12-18 months.
Clinical Findings( Congenital Rubella Syndrome ) May be transient effects in infants. Permanent manifestations may be apparent at birth, become recognized during the first year. Developmental abnormalities appear during childhood and adolescents.
Classical Triad of Rubella Classical Triad Cataract Cardiac abnormalities Deafness Other manifestations Growth retardation Rash Hepatosplenomegaly Jaundice Meingoencephalitis CNS defects lead to moderate to profound mental retardation
Other Neurological manifestions Problems in balance Motor skills in preschool children altered. A rare complication of Pan encephalitis can occur in second decade with Congenital rubella syndrome may progress to death.
Diagnosis ofCongenital Rubella Syndrome Demonstration of Rubella antibodies of IgM in a new born is diagnostic value. As IgM group donot cross the placenta and they are produce in the infected fetus,
Treatment, Prevention, Control No specific treatment is available CRS can be prevented by effective immunization of the young children and teenage girls, remain the best option to prevent Congenital Rubella Syndrome. The component of Rubella in MMR vaccine protects the vaccinated
MMR Vaccine The MMR vaccine is a mixture of three live attenuated viruses, administered via injection for immunization against measles, mumps and rubella. It is generally administered to children around the age of one year, with a second dose before starting school (i.e. age 4/5). The second dose is not a booster; it is a dose to produce immunity in the small number of persons (2-5%) who fail to develop measles immunity after the first dose. In the United States, the vaccine was licensed in 1963 and the second dose was introduced in the mid 1990s. It is widely used in all National, Universal Immunization programmes
Hepatitis C Infection Hepatitis C Virus Non A, non B Hepacivirus
What is Hepatitis C Virus Hepatitis C virus also known as Non A or Non B virus found while doing experiments on Chimpanzees. HCV infections are seen only in humans The epidemiology is like HBV infection.
HCV Virology The virus is not been grown in culture The virus is 50- 60 nm with linear +ve single stranded RNA genome surrounded by an enveloped carrying glycoprotein spikes Now classified as Hepacivirus in the family of Flaviviridae Six genotypes are identified, with high mutability
Hepatitis C Virus RNA-dependent capsid envelope protein protease/helicase RNA polymerase c22 c-100 33c 5’ 3’ NS3 NS5 core E1 E2 NS2 NS4 hypervariable region
Hepatitis C Virus Genome resembled that of a flaviviruspositive stranded RNA genome of around 10,000 bases 1 single reading frame, structural genes at the 5' end, the non-structural genes at the 3' end. enveloped virus, virion thought to 30-60nm in diameter Morphological structure remains unknown
Terminology Family Genus Species Genotype Subtype Quasispecies
Hepatitis C - Clinical Features Incubation period: Average 6-7 wks Range 2-26 wks Clinical illness (jaundice): 30-40% (20-30%) Chronic hepatitis: 70% Persistent infection: 85-100% Immunity: No protective antibody response identified
How HCV transmitted Blood transfusions Transplantation of organs Injectable drug abusers Immunocompromised Sexual transmission ? Vertical transmission is possible
Clinical features Overt Jaundice is seen in 5% of patients About 50 – 80% patients progress to chronic hepatitis May progress to Cirrhosis, or Hepatocellular carcinoma
Chronic Hepatitis C Infection The spectrum of chronic hepatitis C infection is essentially the same as chronic hepatitis B infection. All the manifestations of chronic hepatitis B infection may be seen, although with a lower frequency i.e. chronic persistent hepatitis, chronic active hepatitis, cirrhosis, and hepatocellular carcinoma.
Transmission of HCV Percutaneous IV drugs Clotting factors before viral inactivation Transfusion, transplant from infected donor Therapeutic (contaminated equipment, unsafe injection practices) Occupational (needle stick) Per mucosal Perinatal Sexual
HCV - Occupational Transmission Inefficiently transmitted Average incidence 1.8% following needle stick from HCV-positive source 10 times lower than HBV infection Hollow-bore needles Case reports from blood splash to eye No reports from skin exposures to blood Prevalence 1-2% among health care workers Lower than in the general population
Risk Factors Associated with Transmission of HCV • Transfusion or transplant from infected donor • Injecting drug use • Hemodialysis (yrs on treatment) • Accidental injuries with needles/sharps • Sexual/household exposure to anti-HCV-positive contact • Multiple sex partners
Biochemical Indicators of Hepatitis C Virus Infection • In chronic hepatitis C, increases in the alanine and aspartateaminotransferases range from zero to 20 times (but usually less than five times) the upper limit of normal. • Alanineaminotransferase (ALT) levels are usually higher than aspartateaminotransferase (AST) levels, but that finding may be reversed in patients who have cirrhosis. • Alkaline phosphatase and gamma glutamyltranspeptidase are usually normal. If elevated, they may indicate cirrhosis. • Low platelet and white blood cell counts and raised levels of serum globulins (including immunoglobulins and rheumatoid factor) are frequent in patients with severe fibrosis or cirrhosis, providing clues to the presence of advanced disease. • The enzymes lactate dehydrogenase and creatinekinase are usually normal. • Albumin levels, bilirubin, and prothrombin time are normal until late-stage disease. • Iron and ferritin levels may be slightly elevated.
Hepatitis C Virus Infection Typical Serologic Course anti-HCV Symptoms Titre ALT alanineaminotransferase Normal 6 1 2 3 4 0 1 2 3 4 5 Months Years Time after Exposure
Laboratory Diagnosis HCV antibody - generally used to diagnose hepatitis C infection. Not useful in the acute phase as it takes at least 4 weeks after infection before antibody appears. ELISA test results to be confirmed with Immunoblotting assay
Molecular Methods in Diagnosis HCV-RNA - various techniques are available e.g. PCR and branched DNA. May be used to diagnose HCV infection in the acute phase. However, its main use is in monitoring the response to antiviral therapy. HCV-antigen - an EIA for HCV antigen is available. It is used in the same capacity as HCV-RNA tests but is much easier to carry out.
Prognostic Tests Genotyping – genotype 1 and 4 have a worse prognosis overall and respond poorly to interferon therapy. A number of commercial and in-house assays are available. Genotypic methods – DNA sequencing, PCR-hybridization e.g. INNO-LIPA. Serotyping – particularly useful when the patient does not have detectable RNA. Viral Load – patients with high viral load are thought to have a poorer prognosis. Viral load is also used for monitoring response to IFN therapy.
HCV Treatment α-Interferon Ribavirin Effective in about 50% of cases No vaccine